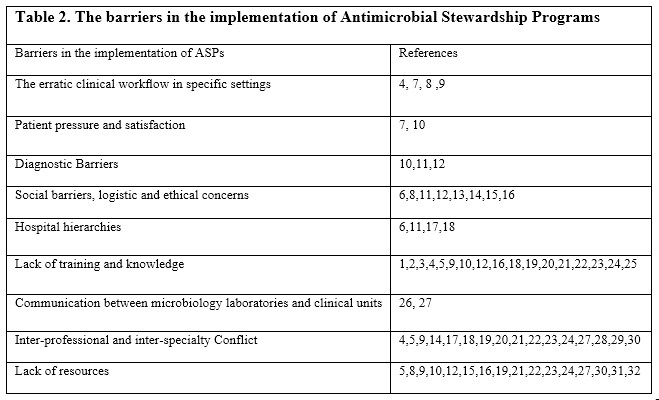
The Barriers in the implementation of Antimicrobial Stewardship Programs
1. The erratic clinical workflow in specific settings such as workload, time constraints, and decision fatigue
The erratic clinical workflow is found in specific settings especially in the emergency department because of the rapid pace in it, which can possibly lead to decrease patient and family participation in the care plan, communication between the health care providers with their patients, and limit the time available for a health care provider for reading and doing research activities (4,7,8,9).
Another obstacle is the increasing workload. If the health care providers are getting tired, the quality of their decisions will be deteriorated (7).
2. Patient pressure and satisfaction
Physicians sometimes prescribe antibiotics for patients, despite disagreeing with the need for antibiotics, to increase patient’s satisfaction and also prevent losing of patients to other physicians for antibiotic prescription (7, 10).
3. Diagnostic Barriers
Another barrier for ASPs implementation are diagnostic barriers. For example, if the causative organism of infection is either virus or bacteria and there is difficulty in diagnosis, it can lead to excessive use of antibiotics (11). In addition to that many long-term care facilities do not have onsite microbiology laboratories and it will also delay the results of organism identification and susceptibility tests (10). Lack of microbiology services is also reported in another study as a barrier (12).
4. Social barriers, logistic and ethical concerns
Social barriers such as perception of resistance, mistrust in antibiotic guidelines, and the skepticism of antimicrobial stewardship importance also affect the application of ASPs. (6, 11, 15) Other studies reported that sociocultural beliefs, logistic barriers, and ethical concerns put impact in the implementation of ASPs (8, 13).
Many pharmacists perceived a logistic barrier to provide clinical support, in particular, the limited communication with other staff, inadequate access to patient’ clinical information, and the logistical issues of off-site General Physicians and pharmacists (14). Lack of willingness to change and perceived loss of prescribing autonomy are other examples reported in other studies (12, 16).
5. Hospital hierarchies
One of the significant prescribing barriers is hierarchical structures (6, 11, 17). The study reported that the hospital hierarchies and consultation etiquette result in conflict between several physicians. For example, in respiratory tract infections, there are conflicts between respiratory specialists and infectious disease specialists. Another example for hierarchical structures barrier is the approval processes which may involve senior physicians to take approval from more junior antimicrobial stewardship physician which is considered as insult (18).
6. Lack of training and knowledge
Lack of knowledge and training can result in inappropriate prescribing of antibiotics (2, 3, 4, 5, 9, 10, 12, 16, 19, 20, 21, 22, 23, 24). One study reported that the lack of knowledge and education for nurses working in respiratory clinics represents a major barrier for the application of ASPs (18). Another study stated that one of the most important problems in the implementation of ASPs is the lack of knowledge regarding the fundamental rules on which antibiotics prescription are based (25). The availability of many clinical guidelines result into lack of knowledge because of the reason that clinicians cannot update themselves with all of these guidelines (1).
7. Communication between microbiology laboratories and clinical units
The poor communication between clinical units and microbiology laboratories is considered one of the main barriers to ASPs implementation. The problems in reporting test results, limited provision of laboratory services and poorly integrated IT systems are examples for this barrier. (26, 27)
8. Inter-professional and inter-specialty Conflict
It is one of the important barriers in APSs and includes conflict regarding the responsibilities for different health care professionals, opposition from prescribers, the communication with antagonizing colleagues, and heterogeneity in the prescribing practices, refuse to accept policies, guidelines about use of antimicrobials, and clinical misconceptions. In addition to that, the limited contact between the health care professionals and the relations between them may compromise on the success of ASPs (4, 5, 9, 14, 17, 18, 19, 20, 21, 23, 24,27, 28, 29, 30).
9. Lack of resources
This barrier includes lack of information technology, audit feedback, guidelines, funding, and lack of human resource.
Lack of information technology included inaccurate or incomplete data access and data extraction. (19, 21, 31). Another barrier is the lack of ASPs electronic surveillance programs and the lack in clinical decision support tools (8, 27). One study reported that lack of guidelines is also one of the important barrier (5, 9, 10). Other studies reported that barriers in the implementation of ASPs include the large volume of audits that are required to assess antibiotic use, lack of resources, enforcement, and specialist support. (12, 16, 27, 32).
Lack of funding and human resource is another barrier reported by several studies (10, 12, 15, 19, 21, 22, 23, 24, 27, 30) in addition to that high level of transient staff (12, 16), the lack of dedicated pharmacy and medical staff (15, 16), and the staffing constraints (15, 27).
Other barriers include lack of leadership (12, 16, 23), pharmacy resources, and microbiology resources (16, 22, 27). Table 2 summarizes the barriers in the implementation of Antimicrobial Stewardship Programs.
{kind=link}
{kind=link}