BBE is an acute immune-mediated neurological disease usually associated with antecedent infection,specifically upper respiratory or gastrointestinal infection[6].The diagnosis of BBE is based mainly on clinical features,although additional examinations,such as anti-Gq1b antibody seropositivity and MRI abnormalities,may contribute to an accurate diagnosis.
Ophthalmoplegia is a core clinical feature of BBE,representing as central nervous system (CNS) involvement in anti-GQ1b antibody syndrome.Gq1b is predominantly expressed at the juxtaparanodes,neuromuscular injections,sensory nerves,and proximal segments of cranial nerves,such as the oculomotor,trochlear,and abducens nerves[7].T2WI and FLAIR images often have high signals,specific localization in bilateral ventromedial nucleus of the thalamus and superior cerebellar peduncle,and also contain a high concentration of GQ1b ganglioside.Neuromuscular block and conduction block caused by autoantibodies against anti-GQ1b binding at these sites can explain ophthalmoplegia,ptosis,and ataxia in BBE.Abnormal signals at specific sites with high anti-GQ1b expression reflected tissue selection specificity.
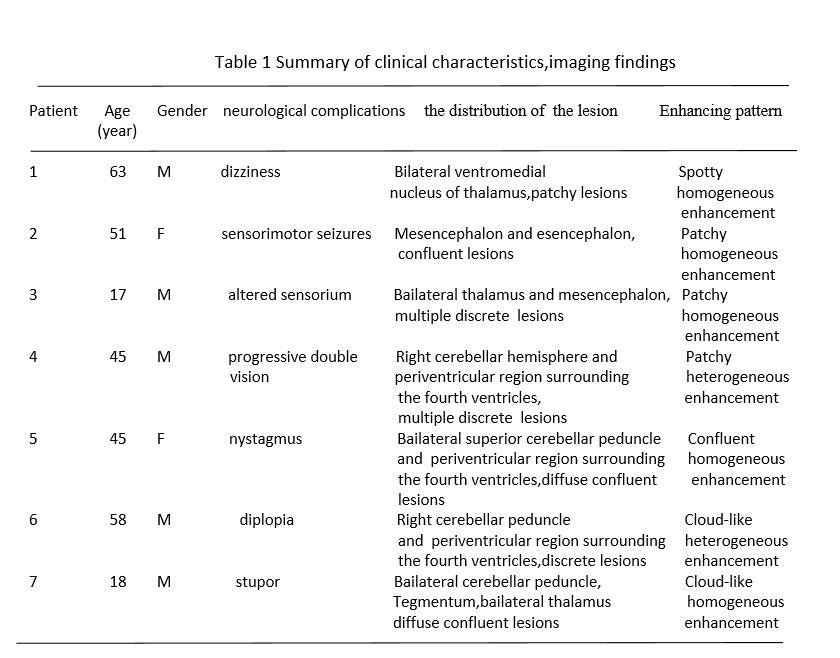
BBE Patients present varying degrees of consciousness disturbance,suggesting impaired brainstem reticular activating system[8].Besides,the detachment of terminal myelin loops may cause the disorder of electrical conduction [9].In our study,MRI showed significant abnormalities involving the bilateral thalamus,mesencephalon tegmentum,and periventricular region surrounding the third and fourth ventricles manifesting hyperintensity on T2-weighted and fluid-attenuated inversion recovery(FLAIR) images.These midline structures are infratentorial sensory circumventricular organs where typical tight junctions among endothelial cells composing the blood-brain barrier (BBB) are anatomically deficient and relatively permeable[10].Similarly,these periventricular endothelial cells that form BBB contain a certain amount of GQ1b,which binding to these sites through circulating macromolecules such as anti-GQ1b antibodies,increasing permeability and allowing macromolecules by inducing BBB breakdown.Electrolytes and free water penetrate the brainstem parenchyma through the endothelial gaps[11].In our study,DWI showed isointense or slightly hypointense,and ADC increase reflected free water in the expanded extracellular space,consistent with vasogenic edema.Diffuse dilatation of extracellular space in the brainstem white matter and leakage of plasma from the vessel alter the brainstem reticular activating system,leading to the development of impaired consciousness.DW images and ADC maps are more sensitive than conventional MRI to determine the extent and degree of vasogenic edema in gray and white matter.
The histopathological process of BBE is associated with the breakdown of BBB which is characterized by dense inflammatory infiltration around the vessels,leading to demyelination and axonal damage[12].Antibody-mediated attacks in the nodes,activating the immunological cascade,and paranode,occurring independently of complement,both results in detachment of terminal myelin loops and disruption of the ion channels and membrane potential[13].In this study,MRS demonstrated that the Cho peak increased and the NAA peak decreased slightly.Cho/NAA values of BBE lesions were within the range.1.01 to 2.41 slight elevation of Cho may result from gliosis or ischemic damage to myelin,while NAA decreases are probably the result of vasogenic edema and neuron cell loss.The increase in Cho/Cr ratio detected in our study indicates that inflammation alone can lead to an increase in Cho levels,which may be secondary to choline oxidase’s input in infiltrating macrophages and lymphocytes.Moreover,the reduced NAA/Cr ratio showed slight axonal degeneration and a reduction in axonal density associated with a decreased NAA values.MRS provides an evaluation of inflammatory demyelinating processes and is a non-invasive means of studying BBE biochemistry.These findings would support a primary demyelinating pathology in the BBE.
However,the exclusion of other disorders may need to be considered,including Wernicke encephalopathy and neuromyelitis optica spectrum disorders.
The distinct MR features of Wernicke encephalopathy are the symmetrical T2WI-hyperintense areas around the third ventricle,the mamillary bodies,and the tectal plate.Mammillary body,periaqueductal gray necrosis were seen in Wernicke encephalopathy.MR demonstrated pronounced cerebellar atrophy with the fourth ventricle’s expansion and marked dilation of the cerebellar fissure[14].
It was found that the longitudinally extensive transverse myelitis (LETM) spinal cord lesion associated with acute myelitis was the most specific neuroimaging feature of neuromyelitis optical spectrum disorders (NMOSD).Other neuroimaging features of
NMOSD shows characteristic periependymal lesions surrounding the third ventricle,involving the thalamus and hypothalamus.Brain lesions in NMOSD are typically localized in the periependymal regions with high expression of aquaporin-4[15].
{kind=link}
{kind=link}