This is a retrospective, single centre, case-control, observational study, whose primary outcome is assessing the impact of a preoperative educational video about the regional anesthesia technique on perioperative levels of patients’ anxiety and satisfaction. The video was previously produced by the Hospital Quality Service as an informational tool to easily explain what intravenous regional anesthesia consists of to patients undergoing elective outpatient hand surgery, as in our institution these patients normally do not meet an anesthesiologist before the day of surgery. A verbal informed consent was obtained from all patients prior to proceed about the use of anonymized data, according to our Ethical Board commission statement. A consecutive cohort of adult patients, scheduled for elective ambulatory hand surgery of less than one-hour duration with an intravenous regional anesthesia (IVRA) over a period of one month after the introduction of the informational video was retrospectively assessed with regard to their level of preoperative anxiety before and after the video and their vital parameters and compared to a consecutive cohort of patients undergoing the same procedures with the same regional anesthesia technique over the month before the introduction of the video. Inclusion criteria were patients older than 18 years of both sex, ASA I-III patients undergoing elective hand-surgery operation and patients anesthetized by IVRA. Exclusion criteria were, on-going anxiolytic or anti-depressive therapy, previous diagnosis of anxiety or psychiatric disorders, recent or regular use of anxiolytic drugs.
Participants and first evaluation
In our institution outpatient hand-surgery patients’ treatment is standardized according to a detailed perioperative protocol. All the patients included in the study underwent a surgical pre-operative visit, during which they received detailed information about the surgical procedure but not the anesthetic technique. Standard allocated time for each preoperative visit was 15 minutes. Patients were than admitted on the same day of surgery to the day-hospital clinic, 2-3 hours before the operation; vital parameters (non-invasive arterial blood pressure, heart rate and respiratory rate) were checked and patients were asked to evaluate their preoperative anxiety level on a visual analogue scale.
Patients of group I were shown the informative video about intravenous regional anesthesia. Patients assigned to the control group (group II) were not shown the video and underwent an otherwise identical preoperative preparation procedure.
After the end of the video and at least 30 minutes before the transfer to the operating room (OR), group I patients re-assessed their own anxiety level. As per every patient, non-invasive arterial blood pressure, cardiac and respiratory frequency were recorded on arrival in the OR and monitored continuously throughout the anesthetic and surgical procedure.
IVRA was performed by an anesthesiologist and a nurse in the induction room outside the OR using a standardized procedure. Two intravenous lines were placed on each hand; after tourniquet inflation, a total volume of 40 ml of chloroprocaine 0.5% was injected intravenously in the operated limb. The patient was then transferred to the OR and 10 minutes after local anesthetic injection, the surgeon tested loss of sensitivity with a pinprick test, after which surgery began.
Visual analogue scale:
The VAS score (Visual Analogue Scale) is a valid instrument used for measuring anxiety33-35. An adapted VAS score (VAS-A), a semi-quantitative visual scale (from 0 – no anxiety - to 5 – maximal anxiety) was used to measure patients’ anxiety levels, asking each patient to subjectively quantify its own anxiety. Other validated scoring systems, like the STAI-score (State Trait Anxiety Inventory score) are not used in our institution due to their greater complexity36.
Educational video:
Patients in the video group watched the video using a laptop and VAS score was repeated after the video. The video was shot by the Anesthesiology department team, in order to explain and show in a detailed and yet easy way the sequence of events that occurs between the arrival of patients in the OR and the performance of IVRA as well as all the steps IVRA consists of. The video began with an actress interpreting a patient scheduled for an elective outpatient hand surgery procedure acceding the day hospital clinic. It showed the interaction between the patient and the nurses who explain in details what is going to happen next and lead her through the preparation routine. The camera then followed the patient as she is accompanied to the induction room and the video showed all the details of the checks made as the patient accedes the operating room, the time-out and the preparation for the anesthetic procedure, with the monitoring of the vital parameters. Than the IVRA procedure was shown in details as an anesthesiologist explains it step by step. The video concluded with the patient being brought to the operating room and staying awake and pain free as a simulated procedure begins.
Feedback questionnaire:
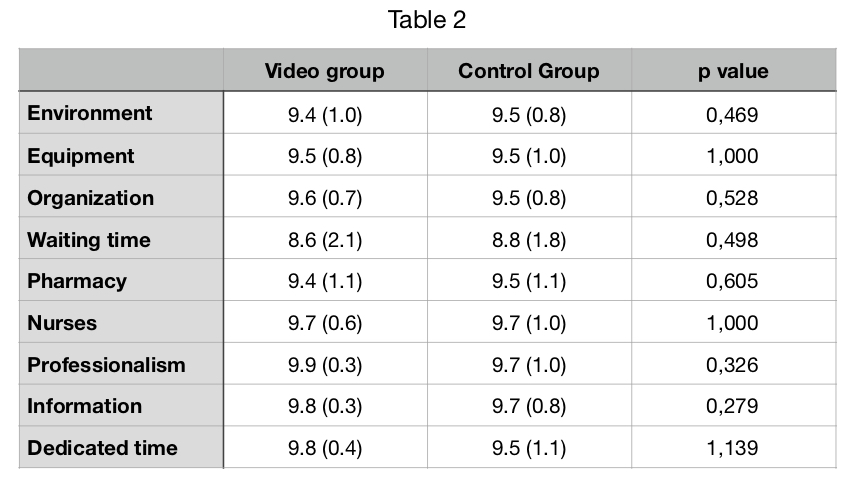
At the end of the surgical procedure all patients were transferred directly to the day-hospital clinic. Between 1 - 3 hours after the operation all patients completed a satisfaction questionnaire with close evaluation from 0 to 10 regarding these topics: environment, equipment, organization, waiting time, pharmacy, nurses, professionalism, information, dedicated time. Moreover, group I patients received a specific feedback questionnaire about the video, in which they were asked about personal satisfaction and video’s education value (‘Was the video a valuable source of information for you?’).
Outcomes:
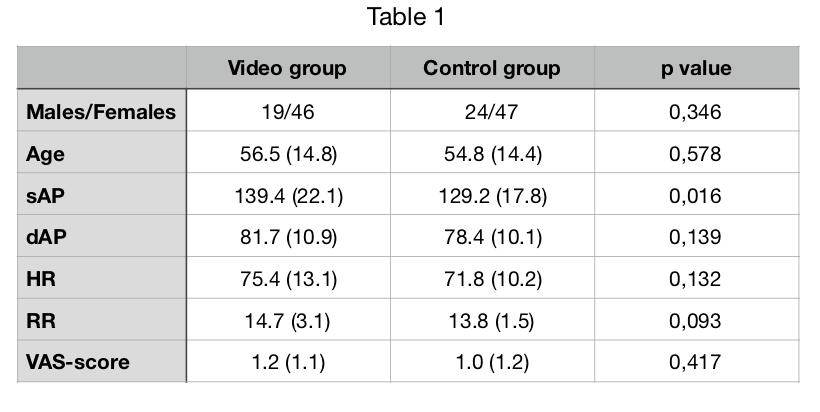
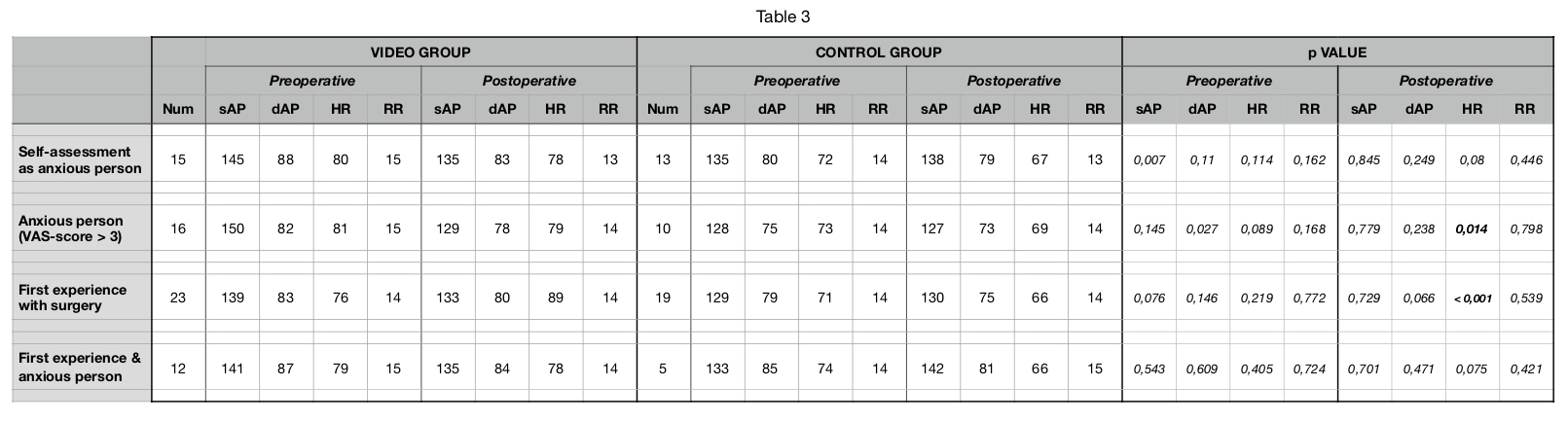
The primary outcome was the difference in preoperative anxiety levels and overall satisfaction levels between two groups measured on a visual analogue scale (VAS-A). Secondary outcomes were differences in in perioperative vital parameters that are usually affected by anxiety (like arterial blood pressure [mmHg], respiratory rate [breath per minute] and heart rate [beat per minute]). All these outcomes were further analysed in subgroups of specific categories of patients, like subjectively anxious patients, objectively anxious patients (with a VAS-score more than 3), patients at their first surgical experience and finally patients objectively anxious at their first surgical experience.
Statistic
A power analysis was conducted. According to Ayral et al37, as well according to estimated clinically relevance of diminution for anxiety, assuming a reduction of at least 50% in preoperative anxiety level as clinically significant, 45 patients per group were necessary (allowing for drop-outs) to reach a 95% level of significance with a power of 90%. We conducted a statistical frequency analysis regarding common vitals parameters and anxiety level according to VAS-scale at arrival in the hospital, before to go to the pre-operative room and at arrival at the pre-operative room, performing a statistical frequency analysis comparing all these three steps and all subgroup according to secondary outcomes. All data were registered and stored in a specific and protected archive in Anesthesia Department, accessible only by the investigators; they were than anonymously transcribed into a database in order to be analysed.
{kind=link}
{kind=link}
{kind=link}