Fig 1 shows a flow diagram of the study selection process. A total of 1,074 records were initially identified from the database search. Of these, 382 records were excluded for duplicates, and 653 records were excluded after screening the titles and abstracts. After full-text screening, a total of 11 studies [6, 16-25] were included in the meta-analysis.
Characteristics of included studies
The characteristics of studies included in our meta-analysis were summarized in Table 1. All 11 RCTs were multicenter studies. Three [16, 18, 19] studies were conducted in multi-countries, while the remaining eight trials were each from France [17], Itay [20], USA [21], Brazil [22], China [6, 23], UK [25], India [24]. Overall, a total of 6,579 patients were enrolled in our meta-analysis, 4,906 of them were male (74.6%), and the average age ranged from 54 to 75 years old. A total of 3,406 were administrated with tocilizumab in addition to standard care or placebo, 14 of which were administrated with tocilizumab and favipiravir, and 3,173 were administrated with standard care or placebo, 7 of which were administrated with favipiravir. Except two [21, 22] RCTs used only a single dose of tocilizumab, other nine [6, 16-20, 23-25] RCTs allowed additional dose if needed. The tocilizumab doses vary from 400 mg to 800 mg and were all administrated intravenously infusion for more than one hour. The maximum dose was 480 mg/d in one study [24], 800 mg/d in eight studies [16-22, 25], 400 mg/d in two [6, 23] studies.
Assessment of risk of bias
There was a high risk of bias in blinding of participants and personnel and blinding of outcome assessment because of open-labelled design in eight studies [6, 16, 17, 20, 22-25], there was an unclear risk of bias in allocation concealment because of no mentioned of allocation in one study [23], shown in Fig 2.
Primary outcomes
Mortality
Nine studies [16-22, 24, 25] with 6,493 patients were included in the meta-analysis. Overall, there was a significant difference between tocilizumab and control groups at 28–30day mortality (RR = 0.89, 95% CI 0.80-0.99, P = 0.04). Two trials with 507 patients contributed to the 60-day mortality, and no statistically difference was found (RR = 0.88, 95% CI 0.54-1.43, P = 0.60), shown in Fig 3.
Incidence of mechanical ventilation
Eight trials [16-19, 21, 22, 24, 25] examined the incidence of MV between tocilizumab and control groups. The pooled analysis including 5,369 participants showed that tocilizumab could significantly decrease the incidence of MV (RR = 0.79, 95% CI 0.71-0.89, P = 0.0001), shown in Fig 4.
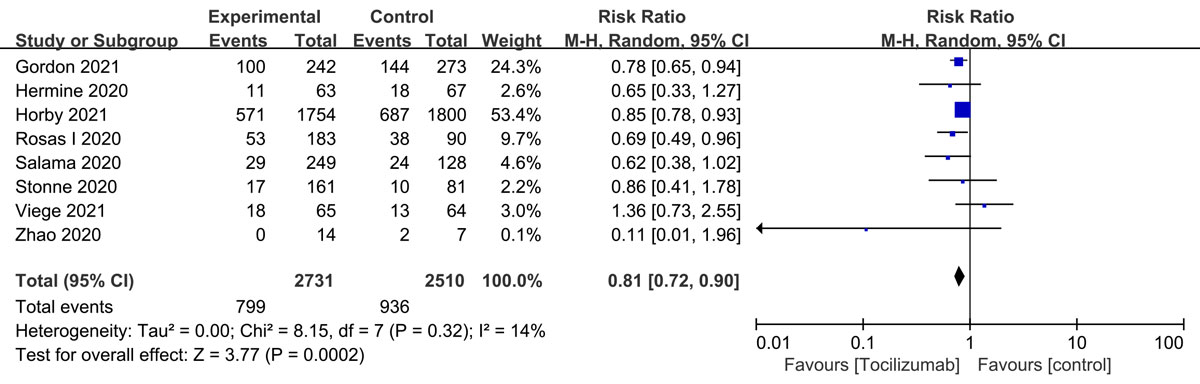
Composite outcome of death or MV
Eight RCTs [16-19, 21-23, 25] including 5,241 adults examined the composite outcome of death or MV. The pooled analysis showed that there was a significant difference between tocilizumab and control groups (RR = 0.81, 95% CI 0.72-0.90, P = 0.0002) (supplemental Fig 5).
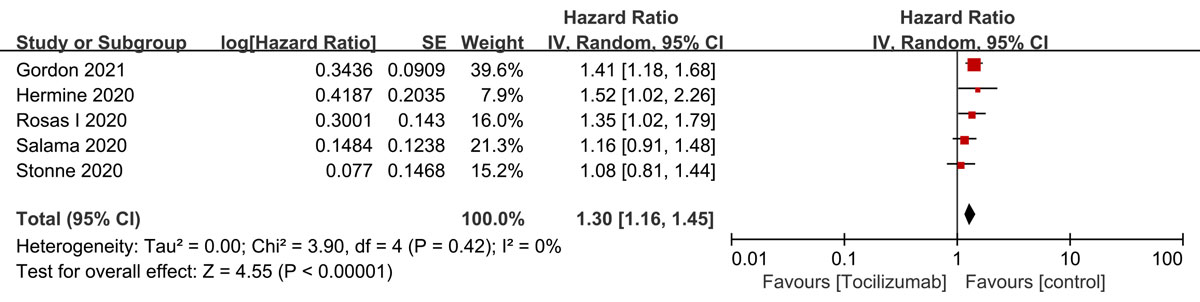
Time to hospital discharge
Pooled analysis of five trials [16-19, 21] with 1,943 cases showed that there was a statistically significant difference in time to hospital discharge between tocilizumab and control groups (HR = 1.30, 95% CI 1.16-1.45, P< 0.00001 ) (supplemental Fig 6).
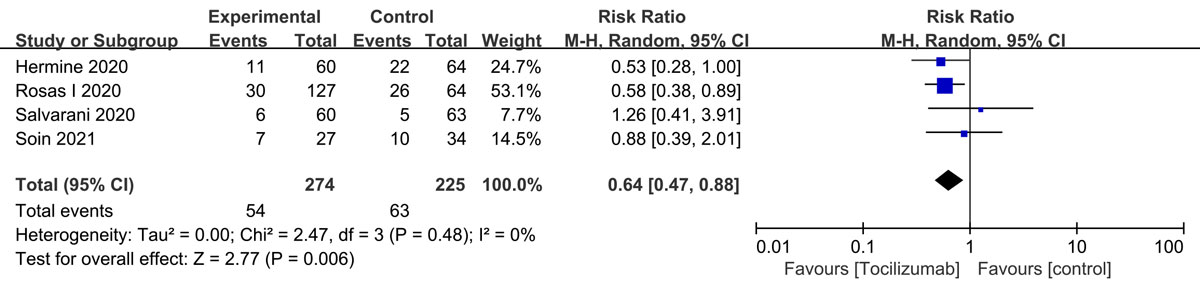
ICU admissions
Four trials [17, 18, 20, 24] with 499 cases were included in the meta-analysis. Overall, there was statistically significant difference between tocilizumab and control groups in ICU admissions (RR= 0.64, 95% CI 0.47-0.88, P = 0.006) (supplemental Fig 7).
Secondary outcomes
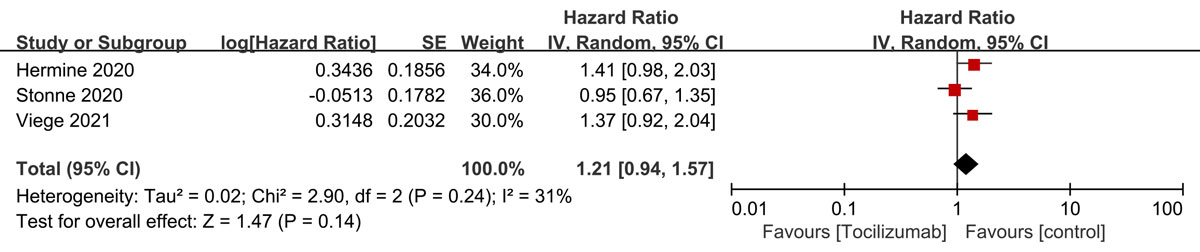
Time to oxygen supply independency
Our meta-analysis including three RCTs [17, 21, 22] with 502 cases showed that there was no significant difference in time to oxygen supply independency between tocilizumab and control groups (HR = 1.21, 95% CI 0.94-1.57, P = 0.14) (supplemental Fig 8).
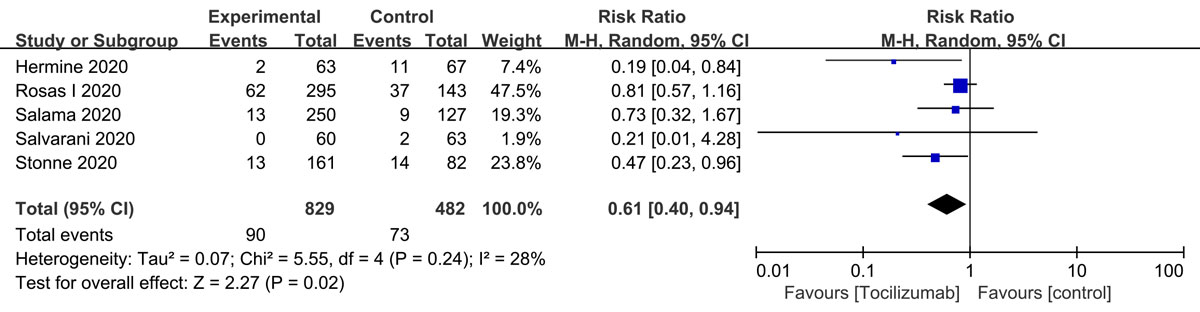
Serious infection
Five RCTs [17-21] including 1,311 cases were included in the meta-analysis. Overall, there was statistically significant difference between tocilizumab and control groups in serious infection (RR = 0.61, 95% CI 0.40-0.94, P = 0.02) (supplemental Fig 9).
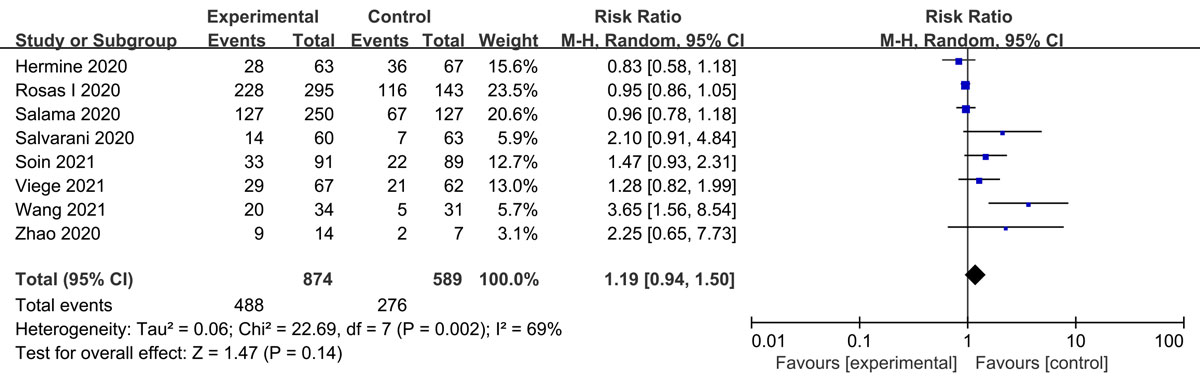
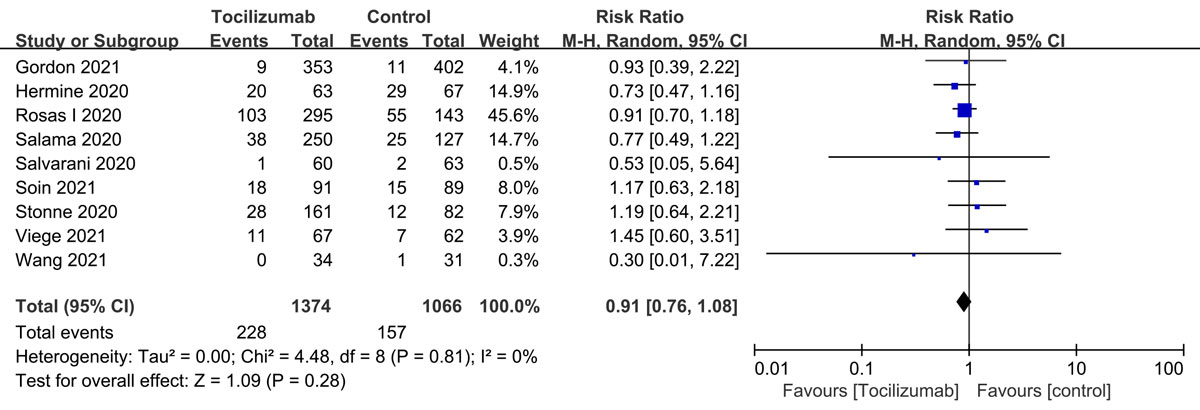
Non-serious adverse events and serious adverse events
Eight studies [6, 17-20, 22-24] including 1463 patients showed that there was no difference between tocilizumab and control groups in non-SAE (RR = 1.19, 95% CI 0.94-1.50, P = 0.14) (supplemental Fig 10). Nine trials [6, 16-22, 24] with 2,440 participants showed that there was no significant difference between tocilizumab and control groups in SAE (RR = 0.91, 95% CI 0.76-1.08, P = 0.28) (supplemental Fig 11).
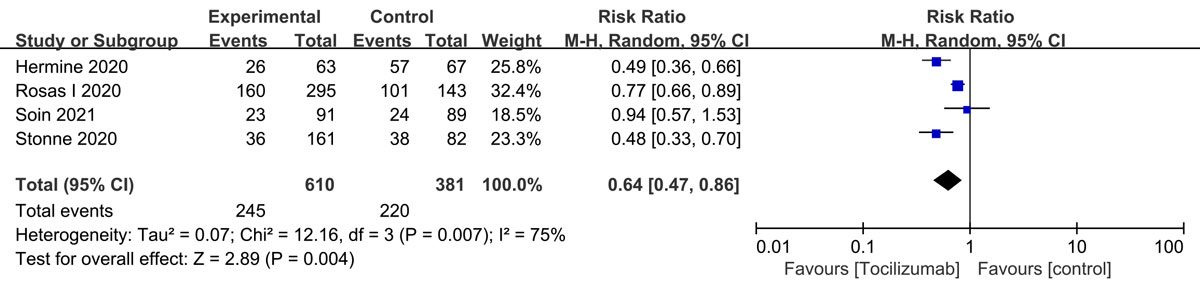
Events of serious adverse advents
Our meta-analysis including four trials [17, 18, 21, 24] with 991 cases showed that there was a significant difference between tocilizumab and control groups in events of serious adverse advents (RR = 0.64, 95% CI 0.47-0.86, P = 0.004) (supplemental Fig 12).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}