Qualitative assessment
A total of 407 participants were included in the workshops; 64% of participants were female, 37% were from community-based organisations, 29% were healthcare providers, 15% worked in government departments, and 19% worked in other types of organisations, such as traditional authorities, police forums, and youth forums. There were 31 participants on average per workshop (range: 12–56). A total of 85 key informants were interviewed, of whom 55% were female, 44% were mine representatives, 19% were workshop attendees, and 38% were other identified stakeholders who had not attended a workshop. Of the 48 stakeholders who were not mine employees, 50% were from the health sector, 27% from community-based organisations, 17% from government departments, and 6% from other organisations.
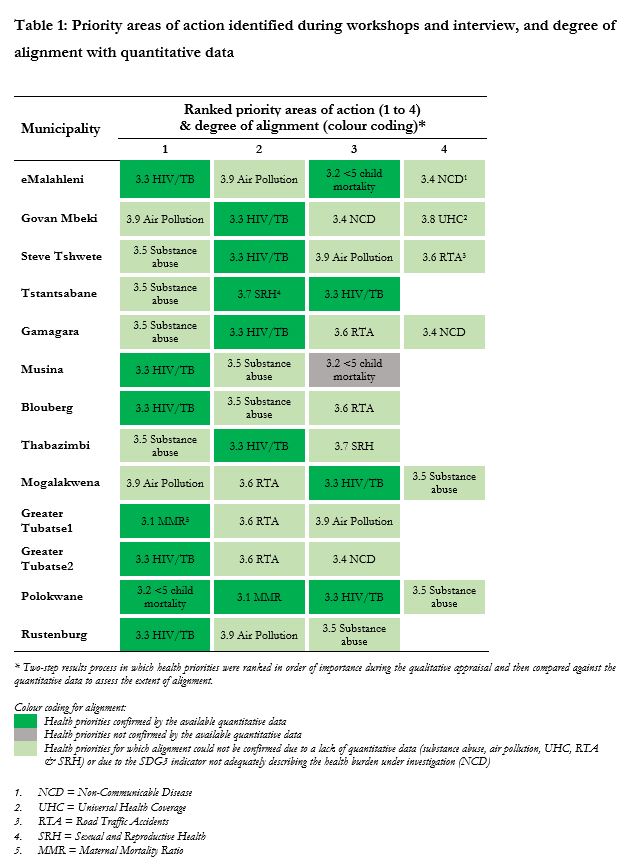
There was a good level of consistency across stakeholders participating in the qualitative assessment, with three key targets emerging for prioritisation: SDG3.3 (communicable diseases), SDG3.5 (substance abuse), and SDG3.6 (RTAs). SDG3.9 (air pollution) was also frequently raised as a possible key target. Table 1 presents prioritised targets based on citation frequency during the workshops and interviews conducted between June and August 2019.
There was a good degree of consistency across workshops and interviews in the reported individual, interpersonal, cultural, societal, and structural factors underlying poor health and wellbeing. It was of interest that despite SDG 3.8 (universal health coverage) only being listed as a priority in the Govan Mbeki workshop, the need for ‘access to quality essential health-care services and access to […] essential medicines’ was raised as a key factor underlying the achievement of SDG3 targets in all workshops. Figure 2 presents a summary of the main factors influencing poor health and wellbeing across the communities.
Quantitative assessment
Quantitative data were available at provincial, district or municipal level for seven of the nine SDG3 targets (3.1 to 3.7), and eleven of the 21 SDG3 indicators (SDG3.1.1: Maternal Mortality Ratio; SDG3.1.2: Skilled Birth Attendance; SDG3.2.1: Under 5 Mortality; SDG3.2.2: Neonatal Mortality; SDG3.3.1: HIV incidence; SDG3.3.2: TB incidence; SDG3.4.1: NCD mortality; SDG3.5.2: Alcohol Consumption; SDG3.6.1: RTA mortality; SDG3.7.1: Family Planning Access; SDG3.7.2: Adolescent Birth Rate). The quantitative assessment generally aligned with the priorities identified in the qualitative data, demonstrating a high burden of HIV and TB (SDG3.3), RTA-related mortality (SDG3.6), and alcohol consumption (SDG3.5). The assessment also highlighted substantial maternal mortality (SDG3.1). Progress towards reducing communicable disease burden (SDG3.3) and maternal mortality (SDG3.1) was found to be poor in most communities. Results arising from the quantitative assessment are presented in detail below.
Qualitative and quantitative assessment alignment
Table 1 presents the degree of alignment between the health priorities identified in the qualitative assessment and the available quantitative data. Although alignment for substance abuse and RTAs could not be confirmed due to insufficient local data, all four provinces were shown to have levels of alcohol consumption above the national average, as well as a higher than average mortality burden due to RTAs. The alignment process for air pollution could not be conducted due to an absence of quantitative data.
Based on both the qualitative and quantitative data, the following five indicators under four SDG targets were confirmed as priority areas for action: SDG3.1 (maternal mortality), SDG3.3.1 (HIV), SDG3.3.2 (Tuberculosis), SDG3.5 (Substance Abuse), and SDG3.6 (RTAs). Figures 3 and 4 present the key quantitative data collected against each of these indicators. We now examine the results for each of these priority areas in turn, drawing out key underlying factors.
SDG priority areas for action
Reduce the maternal mortality ratio to < 70 per 100,000 live births and increase the proportion of births attended by skilled health personnel (SDG3.1)
The qualitative appraisal identified maternal mortality as a priority area for action in Greater Tubatse2, Polokwane, and Govan Mbeki. Teenagers and women living with HIV were identified as being particularly vulnerable. Poor access to healthcare, lack of ambulances, shortage of nurses and homebased carers, lack of health promotion activities, and a lack of antenatal care (ANC) equipment were identified as structural factors impacting on maternal mortality. The key community-level factor was insufficient health education, with individual-level factors including women presenting late for ANC (especially teenagers scared to disclose a pregnancy and unable to access services out of school hours), and poor care pathways leading to women delivering at a clinic different to where they access ANC (sometimes due to denial of a HIV diagnosis).
At 138 deaths per 100,000 live births, the burden of maternal mortality in South Africa remains above the SDG target of < 70. There was a particularly high burden of maternal mortality in Polokwane (352.6), eMalahleni (282.6), and Thabazimbi (156.4) municipalities (see Fig. 3a). As compared to the national figure of 96.7%, five districts had a below average percentage of births attended by skilled health personnel (Gert Sibande: 82%; Nkangala: 87.4%; Mgcawu: 67%; John Taolo Gaetsewe: 79.4%; Bojanala: 76.8%).
End communicable diseases (SDG3.3)
Participants of the workshops and interviews listed this target as a priority area for action in all but one host community. In Greater Tubatse2, this target was prioritised by key informants but not in the workshop, which consisted of a higher proportion of community members than other workshops. HIV and TB were viewed as the most pressing issues impacting on the health and wellbeing, and undermining economic and social development. In relation to the other diseases explicitly mentioned under SDG3.3, malaria was raised as a consideration at a number of sites, mainly in relation to migrants, but there was no mention of Hepatitis B or neglected tropical diseases. Co-infection of HIV and TB was frequently discussed. Adolescent girls, young women, and female sex workers were viewed as particularly vulnerable to HIV, and there were references to the role alcohol and drug use play in terms of HIV transmission, particularly among these populations.
The annual rate of new HIV infections in all districts was higher than the national average of 6.2 per 1,000 uninfected population, which itself is one of the highest new infection rates globally. The HIV data are presented separately in Fig. 4 to indicate that the data are drawn partly from modelled estimates and were collected later. The HIV rate was highest in Gert Sibande at 29.7 new infections per 1000. The annual incidence of TB was above the rate required for TB elimination (in line with SDG targets) in all districts. Rates exceeded the high national burden of 567 cases per 100,000 in Mgcawu, John Taolo Gaetsewe, and Bojanala (see Fig. 3b).
Key structural factors identified as influencing HIV and TB transmission were poor access to quality healthcare and inconsistent access to medication. In-migration was viewed by participants as placing an extra burden on health services. Key societal factors for both infections included poverty, unemployment and food insecurity (affecting treatment adherence). In addition, for HIV, school dropout and a lack of training and recreational facilities for youth were raised, whereas in relation to TB, poor housing, air quality, and ventilation in clinics, transport, and homes were put forward. A key community-level factor was stigma and discrimination for both HIV and TB. Another was socio-cultural and religious beliefs that conflict with prevention, testing and treatment messages (for example, bewitchment; herbal treatment and cures). Interpersonal factors mainly related to HIV, including gender inequalities and gender-based violence, both of which undermine a woman’s ability to utilise prevention methods and increases their vulnerability to HIV exposure. At an individual level, a key issue for TB was access to health education in local South African languages.
Strengthen prevention and treatment of substance abuse disorder (SDG3.5)
The qualitative assessment found target 3.5 to be a priority area for action in all sites. It was perceived as a pervasive and growing problem that required urgent response, with young people seen as particularly vulnerable. Alcohol was reported as the most common substance of harmful use or misuse, followed by cannabis (which is decriminalised), compounds mixed with pharmaceutical products such as methaqualone (a sedative), codeine, and Nyaope (heroin, often mixed with ARVs). Substance use was acknowledged as impacting on SDG3.3 in terms of engaging in high risk sexual activity and hence increased risk of HIV transmission, and on SDG3.6 in terms of being a leading cause of RTAs. Substance use was also perceived to impact on school dropout, child neglect, teenage pregnancy, crime, gang involvement and the perpetration of gender-based violence.
In line with the qualitative results, quantitative evaluation of alcohol consumption in South Africa demonstrated a high average consumption in all provinces under study, as well as a strong gender divide. With the exception of alcohol consumption in women in Limpopo province (1.5 litres of pure alcohol consumed per capita), consumption was higher than the national average for women (2.7L) and men (16.2L) in all provinces (see Fig. 3c). Substance abuse data mainly related to alcohol, and there was no data on the coverage of treatment facilities (an SDG3.5 indicator).
Structural and societal factors influencing substance use overlapped with those influencing HIV and TB, for example, poor access to treatment services, poverty, unemployment, and a lack of youth facilities. Specific to substance use, a lack of law enforcement relating to alcohol policies and illicit drugs was raised. Community factors included stigma (reducing likelihood of accessing support for drug dependence) and socio-cultural norms that glamorise alcohol and drug use. Interpersonal factors included gender-based violence in households headed by people with alcohol or substance use disorder, and children in violent households being vulnerable to harmful substance use.
Reduce the number of global deaths and injuries from road traffic accidents (SDG3.6)
This target was listed as a priority area for action by workshop and / or key informants in ten sites (Blouberg, Mogalakwena, Greater Tubatse, Steve Tshwete, Sishen, Thabazimbi, Govan Mbeki, Tsantsabane, and Rustenburg). Road traffic accidents were strongly associated with concerns about alcohol and drug use. While local-level data was not available, the annual death rate from RTAs was higher (> 21 deaths per 100,000 population) in all four provinces than the national average of 15.9 (see Fig. 3d).
The two key structural factors raised in relation to this target were poor road quality and a lack of traffic and pedestrian safety measures, such as road barriers. Poverty was the key societal factor, with a lack of efficient and affordable private transport (petrol costs) and public transport resulting in a reliance on taxis, whose drivers were deemed to practice poor and risky driving. Expanding the network of ‘scholar patrols’ who help children cross nearby roads to all schools was seen as a priority. At a community level, social norms relating to masculinity were seen to promote poor driving practices such as driving whilst under the influence of alcohol and drugs and speeding, and of being permissive of road rage. Limited first aid experience among community members was equated to a lack of knowledge as to how to stabilise victims of accidents. At an individual-level, poor knowledge of road safety measures, such as driving with lights or walking with reflective clothing, as well as behavioural factors, such as driving impatiently, when tired, and/or when under the influence of alcohol or drugs were raised as concerns.
{kind=link}