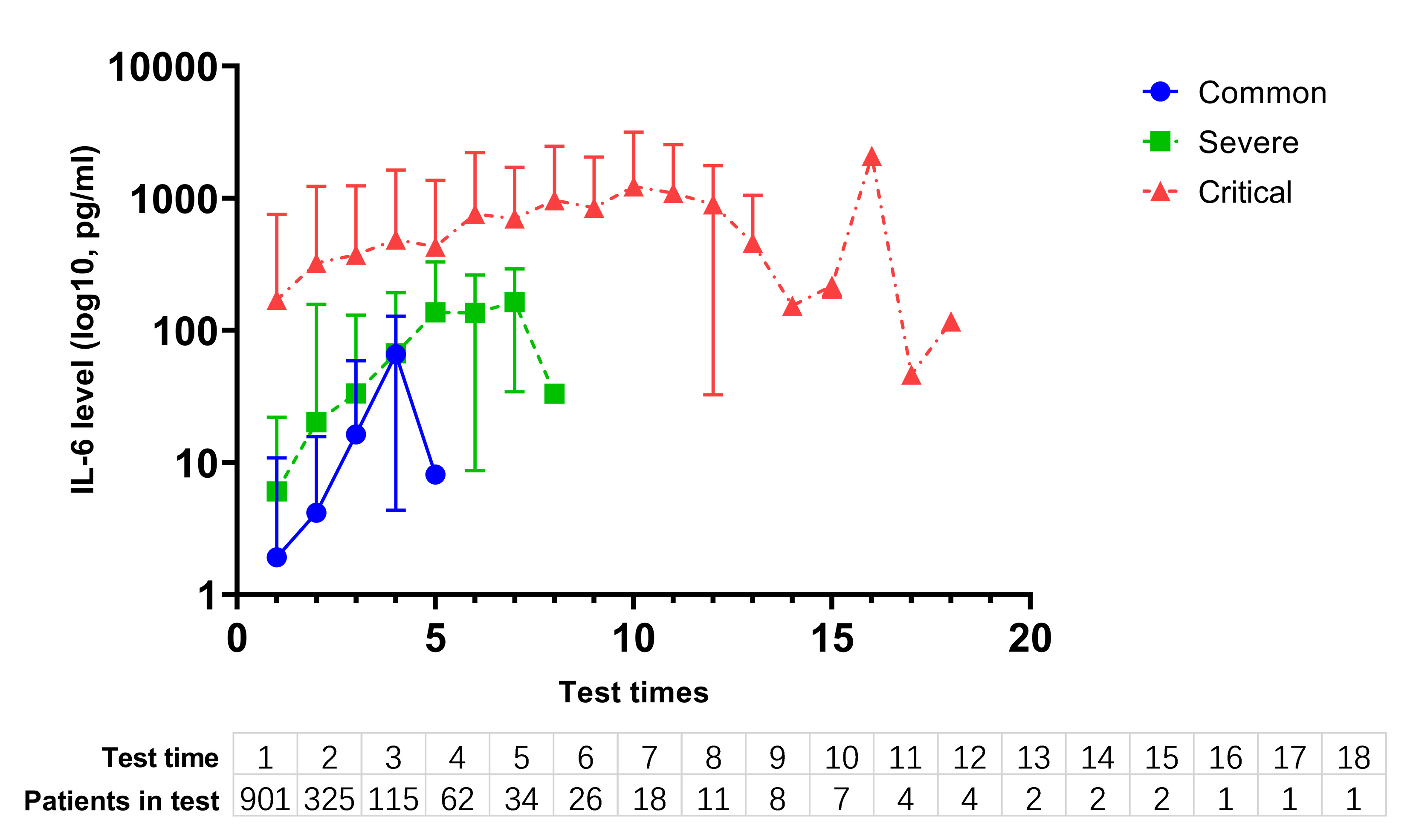
This single-institutional case series describes 901 patients with SARS-CoV-2 infection and symptoms ranging from common to critically ill. Serum IL-6 concentration was tested and analyzed in all the patients. The IL-6 level was tested multiple times in patients with consistently high levels of IL-6 to obtain kinetics profiles. It is increasingly recognized that excessive, malfunctional host immune response may play an important role in the development and maintenance of critical stages of COVID-19. Some teams had reported IL-6 expression in COVID-19 patients, suggesting that elevated IL-6 and other cytokine levels correlated with severity of this disease, however, only a few patients (21–100) were enrolled in these studies (7, 11, 12). Though our result was consistent with that of these studies, this large-sample study gives general profiles of baseline IL-6 distribution among patients with common, severe and critical subsets, suggesting a strong correlation between IL-6 level and severity of COVID-19.
However, correlation does not guarantee causation. Drastically elevated IL-6 levels (> 100 pg/ml), were closely associated with detectable serum SARS-CoV-2 viral load (13). Nevertheless, the bridge between IL-6 and virus is yet to be built. A study related to SARS-CoV (14) revealed that anti-spike IgG abrogated the wound-healing response and promoted proinflammatory cytokines production (IL-8, IL-6, etc.), therefore mediated acute lung injury. This finding implied that IL-6 receptor blockade might be potential way to mitigate lung injury. Nevertheless, some issues are still to be addressed. Proinflammatory cytokines including IL-6 are universally elevated in sepsis and other infections. Zhao et al. (15) compared IL-6 levels between COVID-19 patients and other pneumonia patients, and found that they did not differ significantly (19.34 pg/ml versus. 15.06 pg/ml, P = 0.7). In sepsis, these cytokines played a minor role for their short half-life (16). Besides, IL-6 was shown to be elevated to over 1000 pg/ml in patients with sepsis, even higher than half of the critically ill COVID-19 patients in our cohort, but acute lung injury was not more common in sepsis than COVID-19. According to our kinetics results, we suggest that the duration alongside with the level of IL-6 elevation might play an important role in the severity of disease.
A systemic review conducted by Coomes et al. showed that IL-6 was associated with adverse clinical outcomes (17). Moreover, some studies indicated that different IL-6 cut-off values showed distinct clinical significance. Yong et al. identified the cut-off value of 24.3 pg/ml of IL-6 combining with D-Dimer for early detection of severe cases in a cohort of 43 cases (8). In another cohort in Munich, elevated IL-6 (> 80 pg/ml) was strongly associated with a 22 times higher need for mechanical ventilation compared with patients with lower IL-6 levels in a cohort involving 40 patients, suggesting that high IL-6 level might predict the critical illness (18). In accordance with these previous studies, we found that a cut-off of serum IL-6 (37.65 pg/ml) predicted death with high sensitivity and specificity.
In this cohort, we observed that the IL-6 levels were not necessarily decreased in the patients who are discharged or cured. This is quite different from the result reported by Gong et al., which suggested that higher IL-6 levels in the disease course might indicate disease deterioration (12). Our data appears in contrast with this suggestion since in our study after tocilizumab administration patients might have higher IL-6 levels than before. This phenomenon was also observed in the tocilizumab management of cytokine release syndrome induced by chimeric antigen T (CAR-T) cell infusion, rheumatoid arthritis, and Castleman disease (19, 20). The exact reason for the significant increase of serum IL-6 after administration of tocilizumab is still unknown. One of the potential explanations involves the restriction of receptor-bound IL-6 consumption (19). Furthermore, a transient rise in IL-6 levels might increase the risk of CAR-T-cell-related encephalopathy syndrome (20). Whether higher IL-6 levels resulted from administration of tocilizumab in COVID-19 patients with elevated baseline IL-6 will lead to central nervous system symptoms or other adverse events is worth further exploration, since tocilizumab might be difficult to penetrate the complete blood-brain barrier and then block the IL-6 signal in the brain.
Xu et al. reported the first results of tocilizumab treating COVID-19 in a retrospective study (10). 20 patients were enrolled and after tocilizumab administration clinical symptoms and laboratory indicators were improved in most patients. However, in our study in a similar clinical setting, tocilizumab failed to demonstrate its efficacy in regard to survival outcome under the examination of propensity-score matching design. As a proinflammatory cytokine, IL-6 is pyrogenic. Blocking its receptor, it is predictable that body temperature might decrease, and respiratory distress might be relieved to some degree. However, we expect more than symptomatic treatment of tocilizumab in COVID-19. The survival outcome is pending until prospective, randomized, double-blind clinical trials can be performed.
This study has several limitations. First, this was a retrospective study, however single center might not be a disadvantage since the therapeutic strategy and laboratory tests might remove obvious heterogeneity amongst different centers. Second, due to the nature of compassionate use, characteristics were unbalanced in patients who received tocilizumab or did not receive it. Despite balancing with propensity-score match, unforeseen variables might be left unbalanced as well, which could compromise the rigidity of the results. Third, generally speaking, tocilizumab was administered in severe or critical patients, however, several common cases with moderate elevated IL-6 level received tocilizumab, which might impact the results.
{kind=link}