In this study, we treated patients with locally advanced MSC using external beam irradiation combined with superselective IA chemotherapy, and the 5-year LC and OS were 67% and 50%, respectively. Our results were similar to results in other studies [5, 6]. The combination of IA chemotherapy and external radiation therapy or proton therapy can improve LC and OS [7, 13]. Homma et al. reported good results for 5-year LC (66%) and 5-year OS for stage cT4a (67%) and cT4b (57%) after external radiotherapy and IA chemotherapy [6]. Zenda et al. reported a 1-year LC of 77% and a 5-year OS of 55% for unresectable paranasal sinus and nasal cavity cancers after proton therapy [13]. ENI was not conducted in these studies, including ours, for cN0 cases.
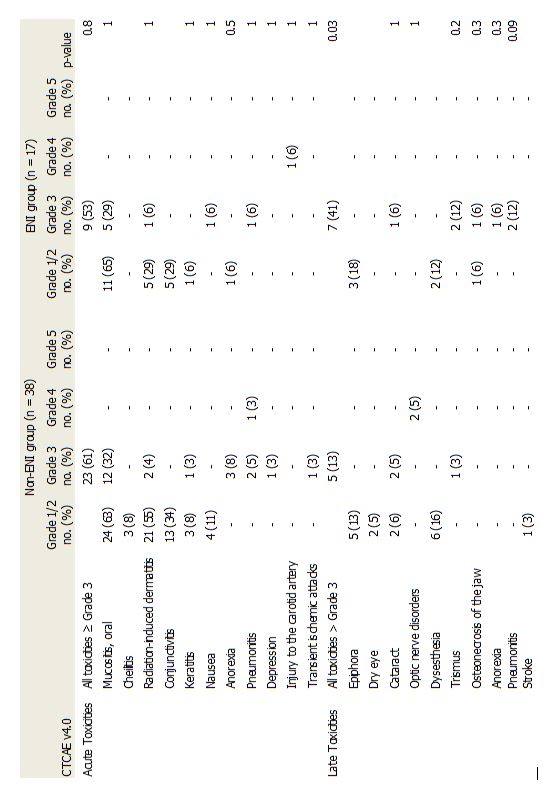
Two of 17 patients with pN + who received ENI in this study developed regional node failure. This incidence was similar to that of patients with cN0, who did not receive ENI. In addition, the 5-year DMFS and 5-year OS in both groups were similar (Table 3). However, there were more patients with high-grade late AEs in the cN + and ENI group than in the cN0 and non-ENI group (41% vs. 13%, respectively; p = 0.03). Feng et al. reported grade 3 dysphagia in 8% of cases and aspiration on videofluoroscopy in 44% of cases 3 months after irradiation with a high radiation dose (mean, 64 Gy) to the pharyngeal constrictor muscle [14]. If ENI is performed for all patients with T3 and T4 disease, the incidence of late high-grade adverse events may increase with prolonged survival [15]. Therefore, it is necessary to select appropriate candidates for ENI to maximize the clinical benefit in locally advanced MSC.
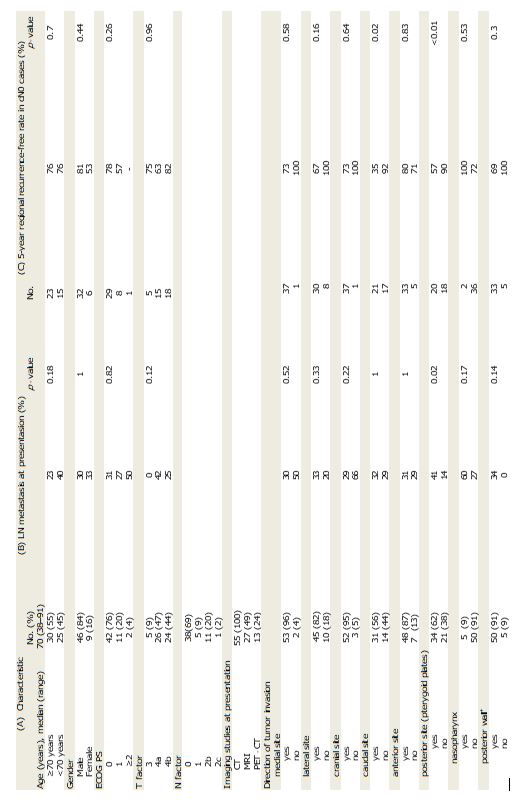
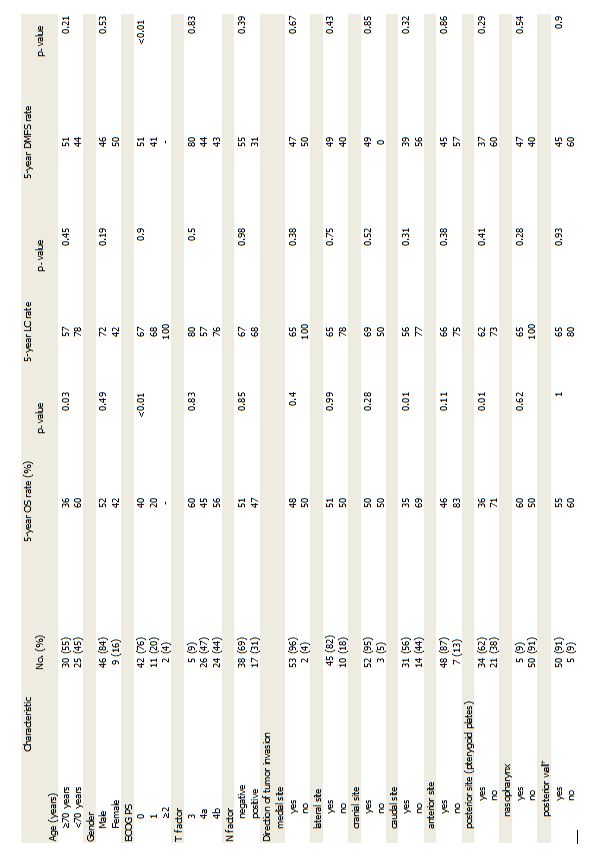
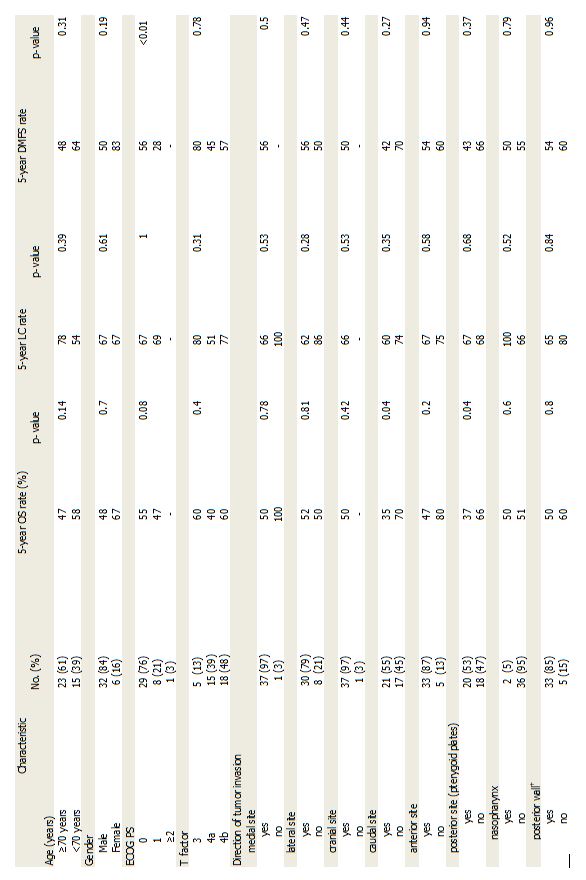
We divided tumor invasion into six directions, and found that only posterior and caudal extension correlated significantly with regional failure. Jeon et al. divided extra-maxillary sinus involvement of the tumor into four directions, and in their definition, destruction of the posterior wall meant infratemporal fossa involvement. The authors reported that this destruction was a significant risk factor for regional failure in cN0 MSC [11]. The categorized destruction of the posterior wall in Jeon et al.’s study meant a wide range of extensions, including T3 and T4 tumors. We attempted to analyze the relationship between the incidence of regional recurrence and the direction of the tumor invasion according to Jeon et al.’s classification. We identified 33 patients with destruction of the posterior wall; however, we found that this was not a significant predictive factor (P = 0.3). Therefore, we divided Jeon et al.’s classification of the posterior wall destruction into two categories: lateral extension (to the masticator space) and posterior extension (to the pterygoid plates) to identify more appropriate risk factors for regional failure. Previous studies reported that ENI for cN0 cases is necessary only if the tumor extends to a contiguous area, such as the nasopharynx or oral cavity, where lymphatic flow is rich [9, 10]. In those studies, regional failure occurred in only T4b cases of nasopharyngeal invasion; only two cases showed nasopharyngeal extension in our series. Invasion of the pterygoid plates is categorized as T4a. All nasopharyngeal invasions were included in the classification of posterior extension, in our study, because tumors reach this region via the pterygoid plates. In this study, the incidences of posterior wall destruction, invasion of the pterygoid plates, and nasopharyngeal invasion were 33 (87%), 20 (53%), and 2 (5%) of 38 cN0 cases, respectively. In our study of advanced MSC (91% of patients were cT4), most cases had destruction of the posterior wall.. Therefore, invasion of the pterygoid plates and oral cavity were considered more appropriate risk factors for regional recurrence. We were able to identify patients with a higher risk of regional recurrence more precisely using our new categorization of tumor extension. Regional failure affects distant metastases and OS [4, 11, 16, 17]. We did not perform ENI for cN0 patients, so its usefulness is still unknown. However, according to our analysis of the risk factors for regional recurrence and OS in cN0 cases (Table 4), these patients were considered good candidates for ENI.
To confirm our results, we also examined the risk factors for LN metastases present at diagnosis in the cN + group. Invasion of the pterygoid plates was the only factor correlated with LN metastases, which supported the results in the cN0 cases. In a multi-center retrospective study by Homma et al., the incidence of LN metastases was significantly higher in cases of nasopharyngeal or oral invasion at presentation among 128 cases of T4 MSC [18]. In all cases of nasopharyngeal invasion, invasion of the pterygoid plates was also observed, which is consistent with our results. Other factors, such as T-stage, PS, or age, showed no association with regional failure.
Regional failure occurred mainly at levels I and II in this study, as reported previously [1]. However, recurrence was also observed in level III in both cN0 and cN + cases. This may be due to differences between IA chemotherapy and systemic chemotherapy. IA chemotherapy is effective only in the arterial perfusion territory; therefore, this method cannot eradicate tumor cells located in the regions far from the primary tumor.
The median irradiation dose to the primary site and LN metastases in our study was 60 Gy, which is lower than the dose in other studies [3, 5, 6]. Previous studies reported high frequencies of the high-grade late adverse event of optic neuropathy (35%) when combining irradiation therapy with IA chemotherapy. Compared with these results, the frequency in our study was relatively low (2/55), and this may be due to the lower radiation dose. Further evidence of the usefulness and optimal procedure for IA chemotherapy will be obtained by an ongoing Phase III clinical trial (University Hospital Medical Information Network (UMIN) Clinical Trials Registry number: UMIN000013706).
This study has several limitations associated with its retrospective design. First, the diagnostic imaging modalities performed before and after treatment were not standardized. Second, when regional failure was suspected, pathological examination was not performed in all cases; 3/9 cases were diagnosed according to imaging findings. Third, differences between IA and intravenous chemotherapy might have affected regional control.
In conclusion, ENI for advanced MSC increased the incidence of severe late toxicities. Invasion of the pterygoid plates and oral cavity were high-risk factors for regional failure in cN0 cases, and these patients may be suitable candidates for ENI.
{kind=link}
{kind=link}
{kind=link}
{kind=link}