Minimally invasive pyeloplasty is the gold standard for treatment of uretero-pelvic junction obstruction. Clinical outcomes are excellent with the improvement observed in 85–100% of patients. Similar results have been shown for different surgical approaches as well as for modifications to the original techniques10,12,17. Our study correlates with this data – 88.5% of cases presented the correct urine passage from the renal pelvis into the ureter, confirmed in diuretic renography with F + 20 protocol, and 80.8% of all patients, which is 91.3% patients in symptomatic patients group, reported reduction of pain intensity to the mild level.
In our study group 3 patients did not have furosemide half-clearance time reduced to < 12 min (2 patients - T½ between 12 and 20 min – 12.5 min and 13 min, 1 patient - cumulative curve -T½ - not estimable). Each of these 3 patients, despite not showing expected outcomes, was satisfied with the results, probably because of the reduction in pain intensity, and for this reason they refused to participate in further procedures, preferring to remain under observation. A similar was observed in 18 patients with postoperative hydronephrosis (69.2%). All of these patients were satisfied with the results. In this group every patient had a good outcome (T½ <12 min) in diuretic renography.
Surprisingly, one patient who had reported dissatisfaction after the procedure, because of an insufficient decrease in pain intensity– from 100 to 50 in the VAS scale, had furosemide half-clearance time < 12 min and no hydronephrosis in ultrasound examination of the kidney.
Also, perioperative complications did not seem to have an impact on patients’ satisfaction. Ninety-six percent of patients, including patients who suffered from complications – Clavien-Dindo I-IVb, would agree to another LP on the other side, if the indications occurred.
Surprisingly, the health domain score assessed in the WHOQOL-BREF questionnaire was only moderate (average 3.5 in 1–5 scale), even though the global QoL score was good (average 4 in 1–5 scale). This result might have been caused by other illnesses that were not evaluated during our study, but the average age of the study group (39.3 yo) does not support this hypothesis.
Sahai et al. showed that there is no difference between preoperative and postoperative physical QoL among patients who had underwent laparoscopic upper urinary tract surgery for benign conditions. However, there was a significant improvement in mental QoL after the procedure, which is thought to be caused by relief from emotional stress associated with pending surgery8.
In a paper comparing open and laparoscopic nephrectomy it was shown that postoperative QoL return to baseline values after at least 1 year was faster in the laparoscopic group18. In our study postoperative QoL was assessed at least 5-years after surgery. We can safely assume that the effect of patient bias caused by perioperative stress and pain due to the operation is negligible.
The obvious limitation of this study is the size of the research group, which is too small to perform a valuable, multifactorial analysis of the factors affecting the quality of life. We cannot reliably conclude, for example, how the surgical technique and/or the presence of crossing vessels affects QoL.
Low study recruitment rate (26 out of 95) could be caused by a fact that all of the surgeries were done in one of the reference centers, performing the highest number of pyeloplasties in Poland. Therefore, our patients often come from distant locations. Their willingness to participate in the study could be weakened by the need of personal arrival. Also, majority of study patients are young people (average age 31 years). These patients are usually reluctant to undergo control tests in the absence of symptoms.
It cannot be excluded that the reason for the lack of response to the study was the poor treatment result, but it does not seem to be the only and most important reason. The poor outcome of the surgery as a reason for refusal in our study seems to be unlikely, taking into account a high success rate that was shown in previous papers published by the authors10,11,17. However, it is possible that patients who were satisfied with the outcome were more willing to participate in the study conducted by the center where surgery was performed compared to the patients who were dissatisfied.
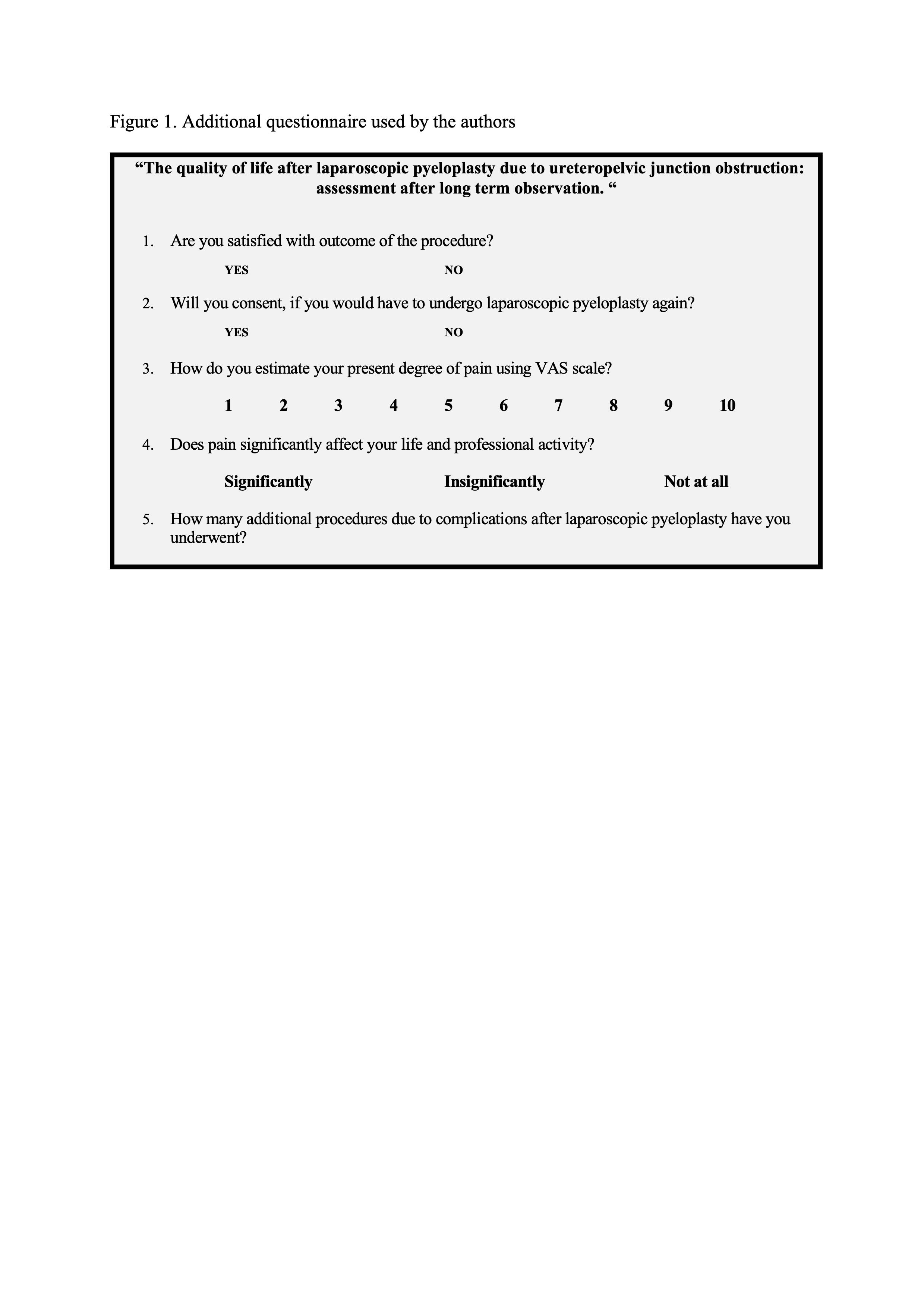
It should also be pointed out that the data regarding preoperative and early postoperative period were gathered retrospectively. Additionally, the test developed by one of the authors and used in the study was not validated. Another limitation of our study is lack of preoperative assessment of HRQoL. WHOQOL-BREF questionnaire and additional questionnaire were given to the patients only in the follow up period. That is why it is impossible to statistically analyze the relation between change in pain intensity and HRQoL.
However, our study seems to be the first one that evaluates postoperative HRQoL post minimally invasive pyeloplasty after long term follow-up. Lack of similar publications makes it difficult to compare our outcomes with the results of others.
{kind=link}