Impaired stretch-induced ANP secretion in the atria from SHR: modulation by subacute treatment with ORS or losartan
Stepwise increase in atrial distension (by elevating atrial fluid levels, 1.1, 2.0, and 2.7 cmH2O, above the basal level of 4.6 cmH2O) resulted in an increase in atrial pulse pressure. Basal levels of pulse pressure were 5.39 ± 0.33, 4.90 ± 0.41, and 4.74 ± 0.78 mmHg, and 4.37 ± 0.47, 4.06 ± 0.52, and 3.60 ± 0.67 mmHg for the first and second runs of WKY-V, SHR-V, and SHR-ORS, respectively (Fig. 1, Aa). Basal levels of pulse pressure between groups were not significantly different. Stepwise increase in atrial distension induced a proportional increase in atrial pulse pressure in all groups, but not significantly in the vehicle-treated WKY. Basal levels of ISF translocation were 22.77 ± 1.35, 21.00 ± 1.81, and 22.80 ± 1.60 µl/min/g atrial wet weight, and 21.99 ± 1.97, 21.11 ± 1.62, and 22.88 ± 0.96 µl/min/g atrial weight for the first and second runs of WKY-V, SHR-V, and SHR-ORS, respectively (Fig. 1, Ac). ISF translocation was increased in response to the elevation of the atrial volume distension in all groups. Basal levels of ANP secretion were 22.77 ± 1.65, 19.84 ± 1.39, and 21.14 ± 1.27 ng/min/g of atrial wet weight and 18.29 ± 0.85, 17.10 ± 1.15, and 20.54 ± 1.80, ng/min/g of atrial weight for the first and second runs of WKY-V, SHR-V, and SHR-ORS, respectively (Fig. 1, Ab). Stepwise increase in atrial distension further increased ANP secretion in the atria from all groups except SHR-V in which ANP secretion was suppressed. Atrial ANP release which reflects the cardiomyocyte release of ANP to the interstitial fluid surrounding the atrial cardiomyocytes [26] was severely affected in the atria from SHR-V. Basal levels of ANP release were 0.335 ± 0.030, 0.305 ± 0.031, and 0.310 ± 0.028 µM, and 0.294 ± 0.035, 0.252 ± 0.026, and 0.297 ± 0.027 µM for the first and second runs of WKY-V, SHR-V, and SHR-ORS, respectively (Fig. 1, Ad). Stepwise elevation of atrial distension increased atrial ANP release but not in the atria from SHR-V. Atrial ANP release was suppressed in the atria from SHR-V. Treatment with ORS reversed the suppressed ANP responses in the atria from SHR-ORS (Fig. 1, Ab and Ad). Atrial effects of ORS on the secretory and dynamic parameters were very similar to those of losartan (Fig. 1B). In the present study, losartan was used as a positive control for the ORS. In the atria from SHR-LOS, atrial distension induced an increase in ANP secretion and ANP release compared to SHR-V (Fig. 1, Bb and Bd).
Summarized stretch-induced ANP secretion in the atria from SHR: suppressed cardiomyocyte ANP release in SHR
Figure 2 depicts the summarized results of atrial distension (stretch of cardiomyocyte)-induced responses in ANP secretion and ISF translocation. Atrial distension was repeated (first and second runs) and the responses were averaged to present as a response to atrial distension in pulse pressure, ISF translocation, ANP secretion, and ANP release (per cent changes over the basal levels) (Figs. 2, 3, and 5) (except pulse pressure in Figs. 2 and 5). Stepwise atrial distension above the basal distension further increased ANP secretion dose-dependently in the atria from WKY-V. Atrial ANP secretion increased by 17.83 ± 3.38, 33.15 ± 6.00, and 65.91 ± 8.10% in response to stepwise increase in atrial pressure by 1.1, 2.0, and 2.7 cmH2O above the basal distension, respectively (n = 8; Fig. 2A). However, distension induced increase in ANP secretion was significantly suppressed in the atria from SHR-V compared with that of WKY-V. (2.72 ± 2.85, 3.43 ± 3.52, and 7.79 ± 4.60% in response to stepwise atrial distension, n = 8; p < 0.004, p < 0.001, p < 0.001 vs. corresponding WKY-V, Fig. 2A). Dose-dependency of the ANP secretion in response to the atrial distension in the atria from SHR-V was also disappeared. Treatment with ORS restored the suppressed ANP secretion and dose-dependency in the atria from SHR-ORS group (22.62 ± 4.20, 33.76 ± 3.28, and 66.89 ± 9.20% in stepwise atrial distension, n = 5; p = 0.002, p < 0.001, p < 0.001 vs. corresponding SHR-V, Fig. 2A). The responses of the atria from SHR-ORS were not significantly different from those of the atria from WKY-V. The effect of ORS on the ANP secretion was similar to that of losartan. Distension-induced ANP release of the cardiomyocytes to the ISF surrounding the cardiomyocytes, the first step of the “two-steps sequential mechanism” of ANP secretion [26], was significantly decreased in the atria from SHR-V compared to the values of WKY-V (-8.02 ± 2.86, -15.86 ± 2.27, and − 20.09 ± 3.62%, n = 8, for SHR-V vs. 8.59 ± 2.81, 15.65 ± 7.14, and 38.12 ± 8.28%, n = 8, for WKY-V; p < 0.001 for all three stepwise increase in atrial distension; Fig. 2B). Treatment with ORS reversed the suppressed ANP release toward the levels of WKY-V (6.76 ± 3.92, 9.12 ± 2.85, and 28.79 ± 1.79%, n = 5, for SHR-ORS vs. SHR-V, n = 8; p = 0.01, p < 0.001, p < 0.001). Effects of ORS on the ANP secretion and ANP release in the atria from SHR-ORS were similar to those of losartan. Taken together, atrial distension significantly increased cardiomyocyte ANP release into the ISF of the atria from WKY-V, while distension-induced ANP release was severely suppressed in the atria from SHR-V. (Fig. 2B). Treatment with ORS or LOS restored the suppressed ANP release in the atria from SHR toward the levels of WKY-V.
Relation between trans-endocardial translocation of ISF and ANP secretion: the role of ORS on the ANP release of cardiomyocytes and cardiac RAS and muscarinic signaling
Pattern of ANP secretion in response to atrial distension was similar to that of ISF in the atria from WKY-V (Fig. 2, A and C). Atrial distension induced ANP secretion is a function of the transmural endocardial translocation of the atrial ISF [25, 26]. However, impaired ANP secretion was not associated with ISF translocation in the atria from SHR-V (Fig. 2, A and C). ISF translocation was not significantly different between groups (9.51 ± 2.14, 16.31 ± 3.44, and 21.13 ± 4.15% in response to stepwise atrial distension, n = 8, for WKY-V; 12.44 ± 2.52, 24.35 ± 3.43, and 38.81 ± 5.90% in atrial distension, n = 8, for SHR-V; 15.16 ± 4.33, 22.84 ± 5.12, and 29.06 ± 6.62% in atrial distension, n = 5, for SHR-ORS. To determine the relation between the ISF translocation and ANP secretion, atrial ANP secretion was plotted in terms of ISF translocation. In the present experiments, trans-endocardial translocation of ISF was similar in the atria from the normotensive WKY-V and hypertensive SHR-V (Figs. 2C and 3B). Figure 3B shows ANP secretion is a function of the ISF translocation in the atria from normotensive WKY-V and SHR treated with ORS or LOS. However, the relation between the ANP secretion and ISF translocation was suppressed in the atria from SHR-V. Further, Fig. 3B shows impaired ANP secretion in terms of ISF translocation in the atria from SHR-V and amelioration of the relation by ORS or LOS. In relation with Fig. 2B and “two-steps sequential mechanism” of ANP secretion, Fig. 3B indicates that suppressed ANP release of the atrial cardiomyocyte may be the cause of the impaired ANP secretion of the atria from SHR-V. Also, distension induced ISF translocation was closely associated with the changes in atrial pulse pressure in the atria from WKY-V and SHR-V (Fig. 3A).
Impaired ACh-induced ANP secretion in the atria from SHR: modulation by subacute treatment with ORS or LOS
ACh is a potent secretagogue stimulating atrial ANP secretion [6, 20–22]. To determine effects of ORS on ACh-induced ANP secretion in the atria from SHR, experiments were performed in perfused beating atria from SHR-V and control WKY-V. Figure 4 shows effects of ACh on the atrial dynamics, ANP secretion, ISF translocation, and ANP release in the atria from WKY-V and SHR-V. ACh (300 nM) decreased atrial pulse pressure (Fig. 4Aa) and ISF translocation (Fig. 4Ac). ACh infusion significantly increased atrial ANP secretion and ANP release in the aria from WKY-V (Fig. 4A, b and d). Infusion of ACh was repeated. ACh-induced ANP secretion was severely suppressed in the atria from SHR-V (Fig. 4Ab), while the ANP response to ACh was recovered in the atria from SHR-ORS. To determine the rate of the atrial cardiomyocyte ANP release to the ISF surrounding the cardiomyocytes, atrial ANP release was measured (Fig. 4Ad). ACh significantly increased ANP release in the atria from SHR-ORS. Similarly, ACh significantly increased ANP release in the atria from SHR-LOS (Fig. 4Bd). ACh-induced increase in ANP release was suppressed in the atria from SHR-V, while the ANP release in the atria from SHR-ORS or SHR-LOS partly recovered toward the levels of WKY-V (Fig. 5, A and B).
Summarized ACh-induced ANP secretion in the atria from SHR
Figure 5 depicts the summarized effects of ACh on ANP secretion in the atria from WKY-V and SHR-V. ACh infusion significantly increased ANP secretion in the atria from WKY-V (Fig. 5A), but the ANP response to ACh stimulation was suppressed in the atria from SHR-V. Subacute treatment with ORS recovered the impaired ANP response to ACh in the atria from SHR-ORS. Similarly, treatment with losartan ameliorated impaired ANP response in the atria from SHR-LOS. Figure 5B shows effects of ACh on the cardiomyocyte ANP release in the atria from SHR-V and modification in the atria from rats treated with ORS or LOS. ACh-induced increase in ANP release was suppressed in the atria from SHR-V, while the response in the atria from SHR-ORS or SHR-LOS recovered toward the levels of WKY-V. ISF translocation was not significantly different between WKY-V and SHR groups.
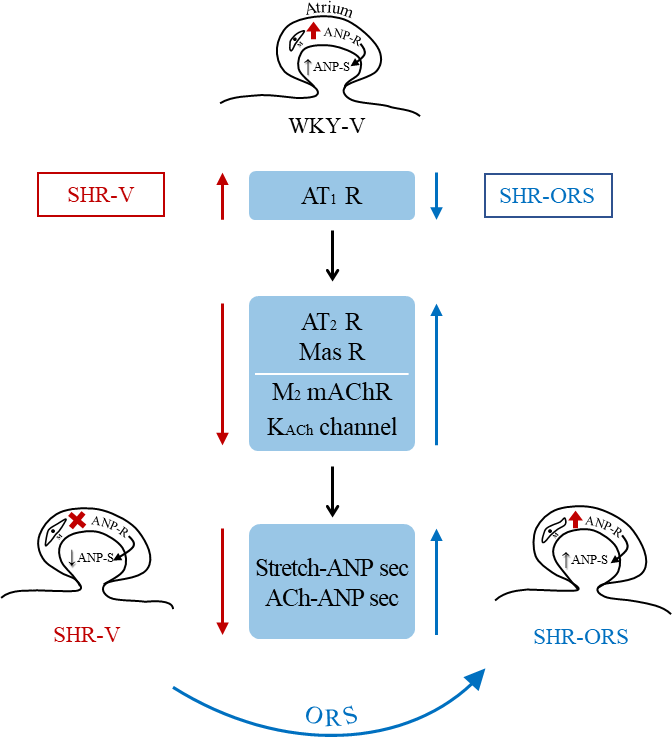
Amelioration of impaired ANP secretion by ORS and the roles of the intracardial RAS and muscarinic signaling in the atria from SHR
Intracardial RAS and muscarinic signaling has been shown to be closely associated with regulation of the atrial ANP secretion [5, 6]. In the present experiments, abundance of the M2 mACh receptor and GIRK4 protein expression was significantly suppressed in the cardiac chambers including atria from SHR-V compared to those from WKY-V (Fig. 6). Subacute treatment with ORS restored the suppressed protein expression of the M2 mACh receptor and GIRK4. The changes were accompanied with the expression of components of the RAS. In the atria from SHR-V, abundance of AT1 receptor expression increased, while AT2 receptor decreased. Treatment with ORS decreased abundance of the AT1 receptor expression, while the treatment increased AT2 receptor. Similarly, AT1 receptor gene expression was accentuated in the atria from SHR-V, while AT2 receptor and Mas receptor expression was suppressed (Fig. 7). Subacute treatment with ORS reversed the expression toward those of WKY-V. The effects of ORS on the RAS gene expressions were similar to those of LOS.
{kind=link}