Breast cancer is the most common neoplasm in women in Mexico (5). INCan and FUCAM have taken on the task of describing the clinical-epidemiological characteristics of the populations they serve; despite this, it is still necessary to explore and understand the behavior of BC in other country regions (4). Three of the most marginalized states of México (Guerrero, Oaxaca, and Chiapas) are in the lowest BC mortality rate in the country (5). This mortality rate is still unexplained; therefore, we have analyzed several prognostic factors that could be related to this and compared them to other regions of the country. Reports from the states of Jalisco, Mexico City, and Veracruz have contributed significantly to the study of breast cancer epidemiology in our country, and the two first had one of the highest mortality rates in the country. The findings of the previous reports give an approximation of the heterogeneity of the disease and outcomes depending on the geographical region analyzed. One of the most relevant characteristics is the age at the time of diagnosis; Rodríguez et al. in 2017 described that in Mexico the mean is 53 years old, lower than reported of populations in developed countries (3). On the other hand, the clinical stage is another important characteristic in the Mexican population: diagnosed patients present more advanced stages, compared to the data published by countries that have early detection programs (3, 6). In Guerrero, the incidence by age group shows a behavior like that described by Rodríguez et al., the average age at diagnosis was 53 years, where the groups with the highest prevalence were 41 to 50 years and 51 to 60 years.
The histological grade is considered a determining factor of the biological behavior of the tumor and a useful prognostic tool. The population presented a greater number of cases with intermediate and high histological grade, both with a similar incidence, as reported by INCan, FUCAM, and the Breast Clinic of the Instituto Jalisciense de Cancerologia (Guadalajara, México) where 90% of the patients presented histological grade II and III (2, 4, 8). Hormone receptors (estrogen and progesterone) and overexpression of the HER-2 oncoprotein are important prognostic and predictive factors (5). According to the 2019 Colima Consensus on Breast Cancer, the classification of the subtypes was established as Luminal A, Luminal B, HER-2, and Triple-negative, while their immunohistochemical approach was Luminal A (HR+/HER2-), Luminal B HR ±/HER2- and HR ±/ HER2+), HER-2 (HR-/HER2+), and Triple-negative (HR-/HER2-) (5). Our subtypes analysis was based on the immunohistochemical approach since it gave us a broad overview of their behavior and allowed us to establish differences between them.
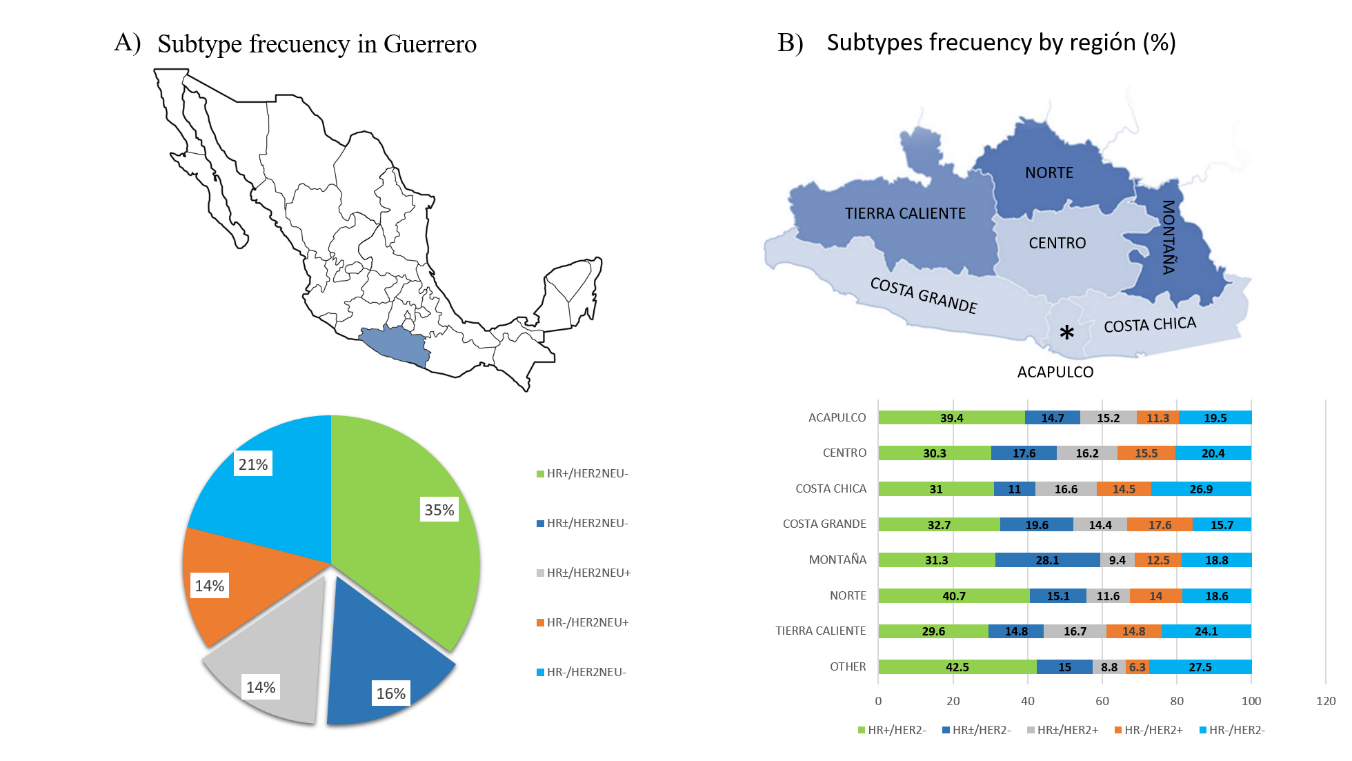
When we tried to contrast our results with data from other's institutions, as INCan, FUCAM, Jalisco, and Veracruz, we found that different workgroups disagree in the reporting of their results; so, to compare them, we standardized the data from different populations according to the Classification of Colima Consensus. In Guerrero, 65.4% of the tumors are of the luminal subtype (HR+/HER2-, HR ±/ HER2- and HR±/HER2+), like Veracruz (65.4%), slightly different from Jalisco (68%) and INCan (60.7%), but not so for FUCAM (76.6%). Regarding the HER2 + tumor subtype, Guerrero, showed a prevalence of 14%, slightly higher than the 9% reported by FUCAM and the 11% in Jalisco and Veracruz, while we observed that HER2 + is more prevalent in INCan (23%). Finally, the triple-negative subtype in Guerrero presented a prevalence of 21% equal to that reported by Jalisco and slightly lower than 23.5% of the cases in Veracruz. Interestingly, the prevalence of the triple-negative subtype in INCan (16%) and FUCAM (15 %) is lower than the data previously cited (2–4, 9)
Comparing our survival results, we found that the median follow-up was 49 months, higher than that reported by INCan (40.5 months), Jalisco (46.8 months), and FUCAM (28 months). The 5-year overall survival in Guerrero was 78% like that reported by Jalisco (78.5%), a percentage slightly lower than the survival reported by INCan (82%) and FUCAM (83%). Regarding survival by subtypes, Guerrero presented 80% survival for the luminal subtype (HR+/HER2 NEU- and HR±/HER2-), lower than that reported by FUCAM and Jalisco, who reported 89%. When these subtypes were individually analyzed, we found that in Guerrero the survival of patients with the HR+/HER2- subtype was 76% vs 84 of the patients who presented the HR ±/HER2- subtype. On the other hand, Guerrero and FUCAM presented the same survival percentage for the HR±/HER2 + subtype, while Jalisco reported 82%. For HER2 + Guerrero showed a 70% survival, this data is like the 69% reported by the FUCAM. Finally, the survival for the triple-negative subtype in Guerrero was 73%, the same as that reported by the FUCAM, while Jalisco reported a 70% survival rate (2–4). The differences in the tumor subtype in our population compared to populations from other states provides important data in the study of tumor heterogeneity.
Most of our patients were diagnosed with advanced-stage breast cancer, this fact can be attributed to the high rate of population marginalization. This condition is evidence of a low educational and health level, where the per capita income is one of the lowest in comparison with the rest of the states of Mexico(10). Other possible causes of these differences can be attributed to the influence of factors such as population aging, the “westernization” of the lifestyle, deficiencies in health education and information, as well as the genetic background of each population (5). Although several factors were included to identify regional differences that could explain the BC lower mortality found in Guererro, the results only display a relatively higher triple-negative frequency in this study in comparison to other reports, but we have not found a difference in survival between patients with this diagnosis. Currently, our country does not have studies that make a detailed description of this characteristic in a particular BC population; understanding the molecular and cellular mechanisms of tumor heterogeneity is relevant in the search for individualized treatments.
In conclusion, the characterization of the clinical-epidemiological profile of each region is essential in the identification of risk and prognostic factors, which are essential in the improvement of strategies aimed at decision making for individualized treatment. In the case of Guerrero, despite the marginalization, most of the epidemiological parameters are shared with other entities in various reports in the literature, only the frequency of the triple-negative being different in the population of this study. Therefore, the BC mortality rates differences are still unexplained and required further analysis; however, it is noted that it is necessary to follow a specific parameters to be able to report breast cancer cases at the national level to make appropriate comparisons at the national and local levels.
{kind=link}