2.1. Patients Study
The study group comprised of 189 adult European Caucasian patients: 85 men and 104 women between the age of 20 and 71 years old. Patients were selected and recruited from the Department of Periodontology at the Medical University of Lublin. After a full explanation of what the aim of this study was, written informed consent forms were obtained from all participants in accordance with the Helsinki Declaration. Medical and dental histories of each patient were gathered: no one had any systemic disease, nor had they taken any antibiotics and/or anti-inflammatory drugs within the last 3 months prior to taking part in the study, neither have they undergone any periodontal therapy in the previous 6 months period. In the study were taken part only non-smoker patients.
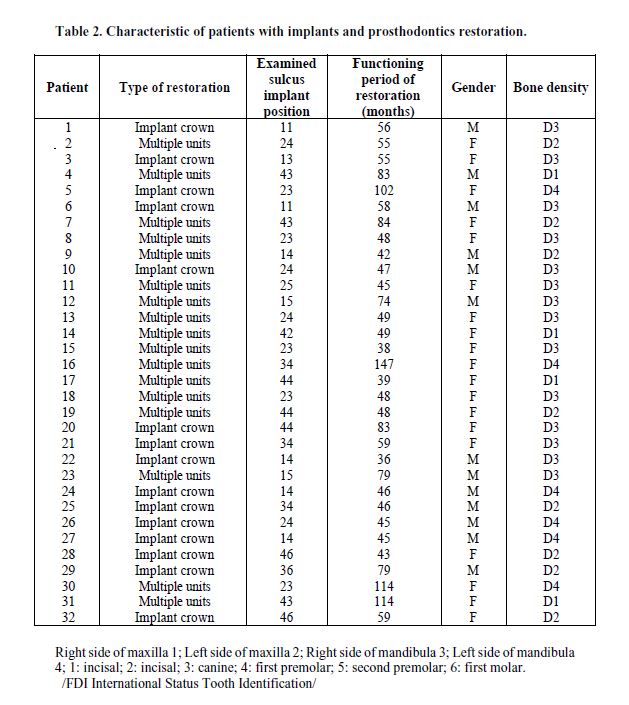
The diagnosis of patients was based on clinical and radiographic criteria. Clinical parameters recorded included gingival index (GI), probing pocket depth (PD), clinical attachment level (CAL), and bleeding on probing (BOP). Both PD and CAL measurements were performed using a conventional periodontal probe. One examiner recorded the clinical data. The baseline characteristics of each study group are presented in Table 1. Based on the clinical data, patients were later divided into five clinical groups as follow: (1) a control group of periodontally healthy patients (13 men and 23 women) with no clinical evidence of gingival inflammation, no radiographic evidence of alveolar bone loss, and PD < 3 mm; (2) patients with mild periodontitis (18 men and 30 women) with PD of 3-4 mm; (3) patients with moderate periodontitis (21 men and 22 women) with PD of 4-6 mm; (4) patients with severe periodontitis (18 men and 12 women) with PD > 6 mm; (5) periodontally healthy subjects (15 men and 17 women) who received an implant treatment (implants with a new alternative hydrophilic surface SPI ELEMENT INICELL, Thommen Medical AG, Grenchen, Switzerland and Brånemark system implant, Nobel Biocare, Gothenburg, Sweden). All patients who had undergone a maxillary implant surgery were subjected to a laryngological examination to exclude, from the study, those with paranasal sinuses disorders and potential complications related to the mentioned conditions. The bone density grade was determined according to a scale of D1-D4 defined by Misch [15]. The examination of implants, including assessment of oral hygiene, PD, BOP, and mobility of implant, was performed. Dental implant survival lasted from 36 to 147 months. In the study group of patients that have received dental implants, none of them showed any symptoms of peri-implantitis. On the other hand, patients that had undergone multiple restorative works presented low clinical mucositis as a result of the prosthetic type used. The characteristics of patients with implants are shown in Table 2.
Periodic clinical examinations were performed for each patient, at least once a year, over 6 to 18 months to assess their bone levels, radiographic images were taken by qualified technicians with the use of the parallel method during each follow-up visit. The bone level (radiographic image analyses) was measured separately by two experienced dentists in a blind test manner who estimated the distance between the alveolar bone crest and the respective tooth cusp.
2.2. GCF/PISF Sampling and Processing
Before a GCF sampling, the supragingival plaque was carefully removed. The collection sites were isolated using cotton rolls and dried with air jets. The GCF samples were subsequently obtained from the mesiobuccal root using sterile Periopaper strips (Oraflow Inc., Plainview, NY, USA) that were overlaid and placed at the gingival crevice region until mild resistance was felt. The strips were left in place for 30 seconds to prevent any mechanical irritation. The strips contaminated with blood were discarded. Following the GCF collection, the strips were kept in sterile test tubes and stored in aliquots at -80°C until needed for analysis.
Clinical examinations in the group of patients with implants were performed after removal of the supra-constructions. PISF samples have been drawn, at least 18 months after the surgery, in a similar way using sterile Periopaper strips that were inserted into the gingival crevice until mild resistance was felt. For 30 seconds the strips were left in place. After that the paper points were transferred to sterile test tube and then immediately stored in aliquots at a temperature of -80°C.
2.3. Cytokine measurements
For GCF/PISF extraction, paper strips were put in tubes containing 500 µL of phosphate-buffered saline (PBS) (pH 7.2) and next gently shaken and incubated at room temperature for 1 hour. After that, the strips were pulled, and the fluids were analysed. Commercially available enzyme-linked immunosorbent assays (ELISA) were used to measure concentration of IL-1β, CXCL8, and TNF (Quantikine R&D Systems Inc., Minneapolis, MN, USA). All ELISA procedures were performed according to the manufacturer’s instruction. All tests were repeated. The GCF/PISF IL-1β, CXCL8, and TNF concentrations were equated to a standard calibration curve.
2.4. Statistical analysis
The statistical analysis for this study was conducted using Statistica 13.1 (Statsoft Inc., USA). Shapiro-Wilk test was used to analyze the normality of distribution, while Mann-Whitney U test was performed to analysed differences in the levels of IL-1β, CXCL8, and TNF in GCF, and differences in the levels of IL-1β, CXCL8, and TNF between G1 and G2 bone density groups, as well. The Spearman's rank correlation coefficient was used to test correlations between IL-1β, CXCL8, and TNF concentrations in G1 and G2 bone density groups. Statistical significance was set at P = 0.05.
{kind=link}