This study developed and validated a nomogram for predicting the prognosis of mCRPC patients who receive ABI and/or ENZ. This nomogram used the initial PSA, initial metastasis status, Gleason score, time to CRPC, previous use of docetaxel or not, age at ABI/ENZ installation, and laboratory data, including the PSA/ALP/LDH at the time of ABI/ENZ installation. The prognosis of mCRPC varies among metastatic lesions. Regarding non-metastatic CRPC (m0CRPC), the PROSPER, SPARTAN, and ARAMIS studies showed the median radiographic progression-free survival (rPFS) to be around 36.6 to 40.4 months [11-13]. Although the final OS was not reached, the OS was expected to be around 67.0 to 73.9 in both groups [14]. Regarding metastatic pre-docetaxel chemotherapy CRPC, the PREVAIL or COU-AA-302 studies showed that the OS was around 32.4 to 34.7 months [1, 15]. Furthermore, regarding metastatic post-docetaxel chemotherapy CRPC, the AFFIRM and COUA-AA-301 showed that the OS was around 14.8 to 18.4 months [2, 16]. Finally, in real-world metastatic CRPC, the OS was found to be 31.6 months in cases of lymph-node metastasis, 21.3 months in cases of bone metastasis, 19.4 months in cases of lung metastasis, and 13.5 months in cases of liver metastasis [17]. While the OS was speculated in metastatic site, the detailed prognostic estimation using multiple risk factors has not been established. To make right treatment decisions for the right patient at right timing, a detailed prognosis estimation is needed.
Previous studies revealed the prognostic factors for metastatic prostate cancer. In terms of tumor markers, systemic inflammatory markers include the neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, lymphocyte-to-platelet ratio, De Retis and prognostic nutritional index, which have all been identified to be prognostic factors for prostate cancer [6, 18, 19]. In addition, either a geriatric assessment or determining the status of sarcopenia have been reported as a new prognostic factor for CRPC [20]. Recent studies have shown that elevated tumor markers, such as LDH and ALP, and some inflammatory markers are poor prognostic factors for CRPC [6]. Zhao et al. developed a prognostic nomogram for CRPC among Chinese patients using a 449-patient cohort [21]. This nomogram used the Gleason score, presence of intraductal carcinoma of the prostate, baseline ALP/PSA/Hb, and the Eastern Cooperative Oncology Group performance status. Yang et al. also developed a nomogram using the presence of liver metastasis, hemoglobin level, and time from initial ADT to ABI in 110 Chinese CRPC patients [22]. Lin et al. developed a nomogram using the PSA-doubling time, time to PSA progression, and presence of pain in 167 Chinese CRPC patients [23]. Similar to other studies, we made nomograms to predict OS in 589 mCRPC patients who received ABI/ENZ. This program facilitated the gathering of important information for both patients and physicians. Though various nomograms have been reported, this program contributed easily approach or daily clinical practices.
In mCRPC treatment, newly established medications are more expensive than ADT or docetaxel treatment, which eventually affects a country’s insurance system [6, 24]. Previous studies also created nomograms to predict the prognosis in Chinese CRPC patients. The economic range in Asia is vast, so nomograms specific to each country are needed. Under the Japanese medical insurance system, all patients received government-approved CRPC medication, including ABI/ENZ, Ra-223, docetaxel, and cabazitaxel. Speleucel T is not approved in Japan. The present findings are expected to benefit Japanese mCRPC patients who are introduced to ABI/ENZ.
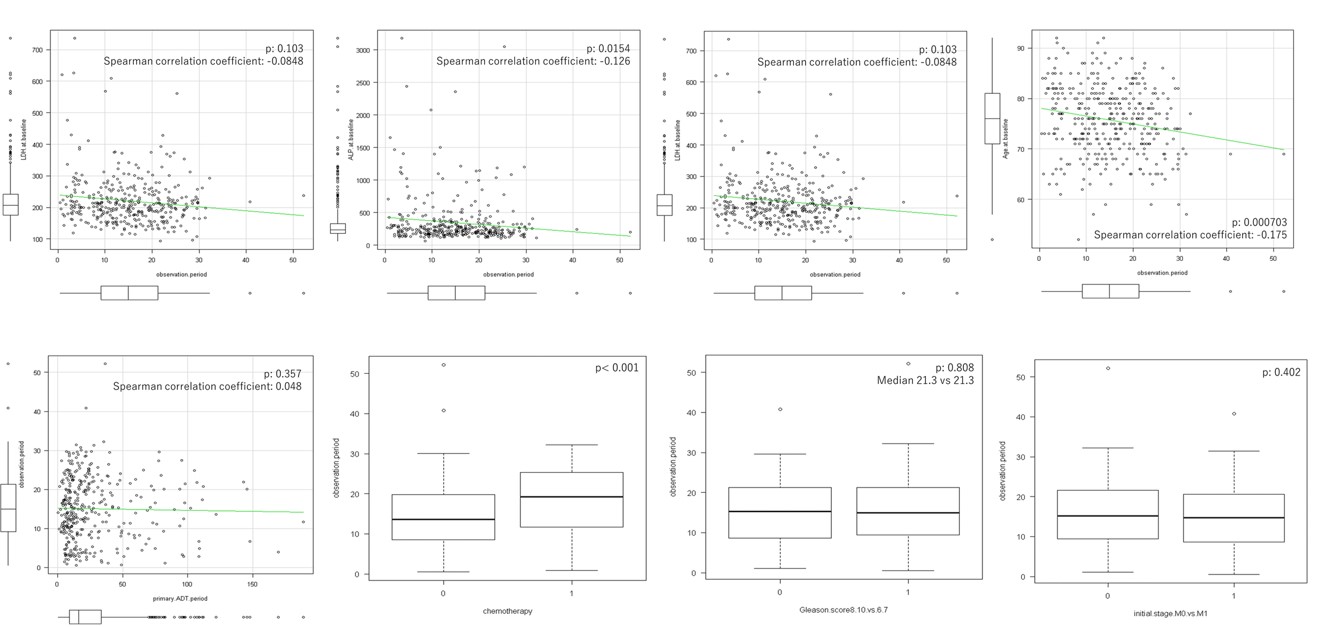
Several limitations associated with the present study warrant mention. First, this study used a retrospective cohort divided into a training group and control group from Japanese multicenter hospitals. Most of the hospitals were third referral cancer centers. Thus, a further study is needed to confirm the accuracy of these findings using all hospitals, including private clinics. Second, other mCRPC treatment drugs, such as PARP inhibitors and immune-checkpoint inhibitors, will be available in the near future. Once these new treatments are approved, additional validation will likely be needed. In addition, this study did not include any upfront treatment for metastatic hormone naïve prostate cancer (mHNPC). Based on the findings of both TITAN and ARCHES studies, upfront apalutamide and ENZ were approved for mHNPC by the Japanese national insurance system in addition to ABI for LATITUDE high risk mHNPC [25, 26]. Further study is needed to confirm the efficacy of this program for the patients who received upfront treatment for mHNPC. The last limitation is shorter observational period. Most patients were followed up for less than 30 months. In this follow-up, 198 (34.9%) patients died and no correlation was observed between the covariates and the observational period [Supplementary fig.1].
In conclusion, we developed and validated a nomogram for predicting the prognosis of mCRPC patients who receive ABI/ENZ treatment using clinical information and also developed app to facilitate clinical usage.
{kind=link}