Polycystic ovary syndrome (PCOS) is a common reproductive disorder, affecting 5–20% of the reproductive-age female population worldwide[1, 2]. In addition, PCOS is associated with ovulatory dysfunction, abdominal adiposity, insulin resistance, obesity, excessive androgen production and cardiovascular risk factors. However, the genetic mechanisms of PCOS remain largely unknown, since the etiology of the disease is very complex and affected both by genomic and environmental factors. Therefore, an improved understanding of the genetic mechanisms of PCOS may provide novel insights into the treatment and diagnosis of PCOS[3].
Polycystic ovary syndrome (PCOS) is one of the most prevailing endocrine disorders with an incidence of 4–21% in women at reproductive age[3].
It is one of the main causes of infertility in women and accounts for almost 75% of anovulatory subfertilities [5]. It has been revealed that both inherited and environmental factors are involved in PCOS [3, 4]. Despite the numerous studies, the exact underlying cellular/molecular mechanisms of PCOS have not yet been understood.
Polycystic ovary syndrome (PCOS), a highly prevalent gynecological disease, is often characterized by amenorrhea, hirsutism, polycystic ovaries on ultrasound scan, elevated serum luteinizing hormone (LH), low serum follicle-stimulating hormone (FSH), anovulatory infertility, pregnancy and neonatal complications[6].Although assisted reproduction techniques (ARTs) are commonly used for PCOS associated infertility, there are still some questions regarding the paucity of high quality oocyte, low fertilization, and fnal pregnancy rate in women with PCOS following ART.In antral follicles, cumulus cells encircle the oocyte to form the cumulus -oocyte-complex (COC). Cumulus cells-oocyte cross-talk plays a very important role in the development,maturity, and fertilization ability of oocyte. In the literature, it has been shown that apoptosis of cumulus cells correlates with poor oocyte outcomes, embryo fragmentation, and impaired blastocyst development[7, 8]. Moreover, it
has been demonstrated that the percentage of apoptotic cells in women who achieved pregnancy was signifcantly lower than that of women who did not become pregnant[9]. Apoptosis is an active process of cellular deconstruction triggered by changes in the levels of specifc stimuli. An apoptotic cell is marked by shrinkage, nuclear chromatin condensation, fragmentation, and budding of the plasma membrane. Finally, the cell turns into apoptotic bodies which contain cell organelles and/or genetic material [10].
Apoptosis of granulosa cells seems to have a negative effect on IVF outcomes. A higher incidence of apoptotic granulosa cells has been related to poor embryo development, and low fertilization and pregnancy rates[11]. PCOS patients undergoing IVF procedure produce a high number of oocytes but approximately, all of them have poor quality leading to poor outcomes[12, 13]. Thus, investigation of the mechanisms of high apoptosis in granulosa cells of PCOS patients is of great clinical importance.
Tumor necrosis factor-alpha (TNF-α) mediates a variety of biological activities by binding to TNF receptor (TNFR) 1 and TNFR2, including cell apoptosis and proliferation[14].TNFR1 is a member of the family of death receptors. The intracellular segment of TNFR1 includes an important and structured domains, namely the death domain (DD)[15, 16], which are required for the induction of apoptosis by TNFR1 ligands.The death domain of TNFR1 is well characterized and mediates homotypic interactions with other death domain-containing proteins. TNFR1 and TRADD interact through their DDs in response to sTNF-α. This interaction is the basis for the formation of two alternative protein complexes (complex I and complex II). Complex I is formed at the cell membrane by recruiting RIP1, TRAF2 and cIAP1/2. This complex leads to activation of NF-κB and promotes cell survival and anti-apoptotic activities. TNFR1 can be also internalized into the cytoplasm, which is dependent on the TRID domain. Subsequently, a second cytosolic complex (complex II) can be formed by the recruitment of FADD and procaspase 8 to the internalized TNFR1-TRADD complex. This complex is called death-inducing signaling complex (DISC) as it is crucial for the induction of apoptosis[14, 17, 18]. In general, the default signaling pathway of sTNF-α is NF-κB pathway activated by complex I at the cell surface. Furthermore, NF-κB activation renders tumor cells resistant to sTNF-α-induced cytotoxicity. However, in case of impaired NF-κB activation the cytosolic complex II is formed, thus switching the pro-survival signaling to pro-death signaling.
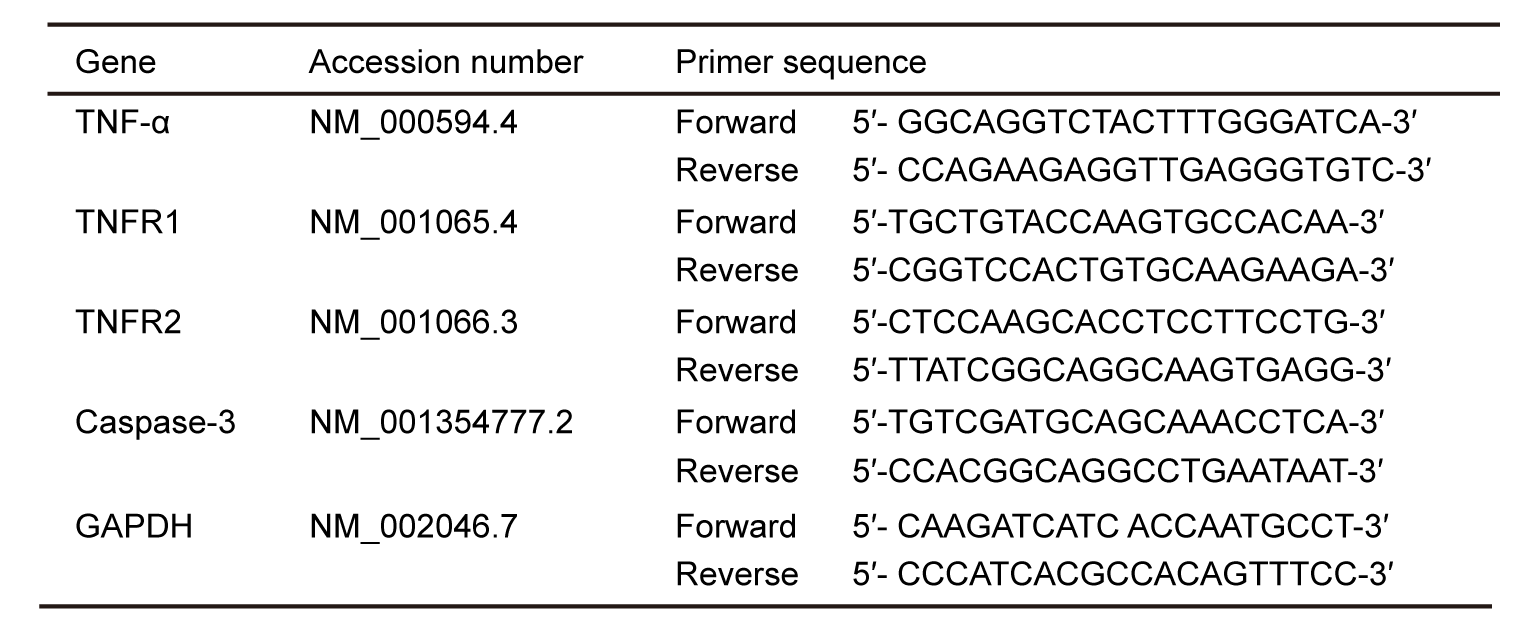
The importance of TNF-α and its receptors has been demonstrated in ovarian function[19]. It has been reported that binding of sTNF-α and TNFR1 in granulosa cells can mediate ubiquitin-mediated phosphorylation and degradation IκB induces NF-κB migration into the nucleus, and activation of NF-κB is associated with XIAP synthesis, thereby promoting granulosa cell survival[20]. The binding of sTNF-α to TNFR1 also promoted the proliferation of granulosa cells by increasing the expression level of c-Jun[21]. However, little is known on the function of TNF‐α in human ovary in PCOS condition. Reports indicate that TNF‐α level was signifificantly higher in PCOS group than control[22], but the molecular mechanisms of TNF‐α signaling pathway in this condition is still unclear. For this reason, we investigated the changes in TNFR1 and TNFR2 expressions in human granulosa cells. We hypothesized that the TNF‐α signaling pathway in human granulosa cells play a crucial role in higher rate of apoptosis in PCOS patients.
{kind=link}
{kind=link}