Patients with severe hemophilia treated with RS using C-Y(90) during November 1998 to February 2017 at the Department of Orthopedics of the Pediatric Hospital, National Medical Center Siglo XXI, IMSS were enrolled in the present study.
The variables collected included place of birth; age at the time of the first C-Y(90) application, weight and height; degree and stage of haemophilic arthropathy. The response of the joint after application of C-Y(90), the number of hemarthrosesper month, the number of doses of factor VIII, IX, and factor VII for patients with inhibitor, number of joints treated, number of patients with inhibitor, joint bleeding-free time and function were also recorded.
To classify the hemophilic arthropathyat each time of C-Y(90) application we used Pettersson score. This is based on typical findings of hemophilic arthropathy on posterior-anterior and lateral X-rays, including osteoporosis, enlargement of epiphysis, irregularity of subchondral surface, narrowing of joint space, subchondral cysts, erosions at joint margins, incongruence between joint surfaces, and the angulation and/or displacement of articulating bone ends. The maximum Pettersson score joint is 13 points indicating more joint damage [10].
The decision to use RS was based on the clinical status of patients at the moment of admission to our department which had been referred from second-level hospitals. None of the patients had received prophylactic treatment and presented recurrent joint bleedings (two or more joint bleeds in one month). They presented signs of progressive arthropathy (being no greater than grade III, according to the Arnold and Hilgartner classification), limited mobility arches and/or an increased joint size or pain.
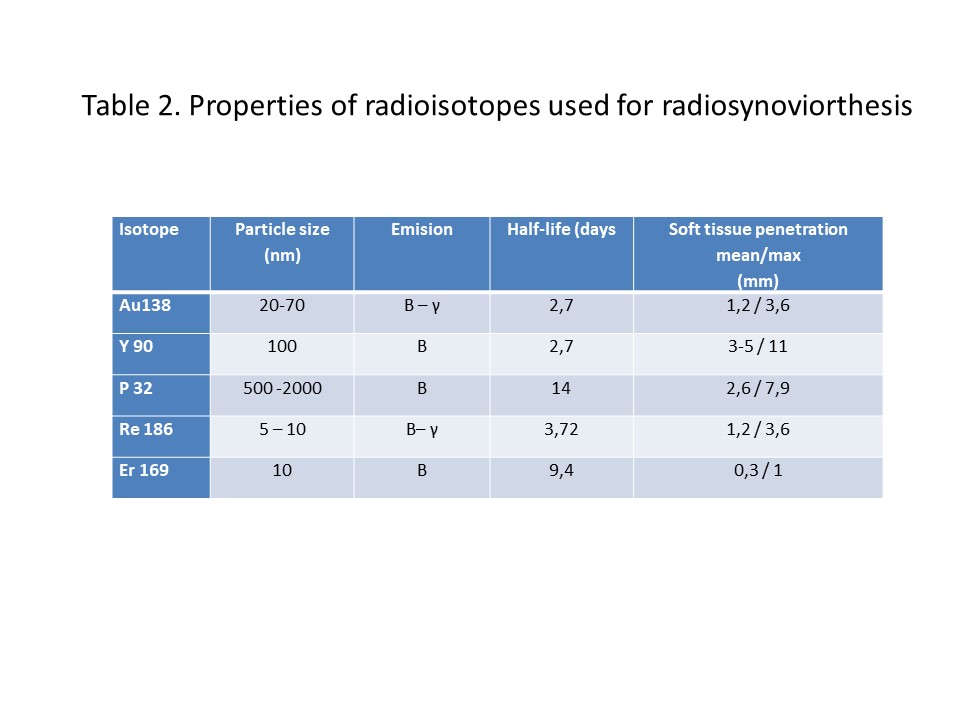
For the RS, different radioisotopes can be used. The selection of the radioisotope should take into account two parameters [4,11]: 1) physical properties: half-life, soft tissue penetration, size of the radiocolloid, 2) and clinical features: joint size, amount of joint fluid, synovial thickness. The material should also be a pure beta emitter, thereby minimizing the whole body exposure to gamma radiation [4, 8,12,13].
Among the available radioisotopes, we chose C-Y(90) taking into account their physical properties and clinical characteristics, as well as the good results obtained with RS with this medication published in the literature in pediatric patients.
All patients received replacement therapy to cover the procedure with FVIII and FIX except those with inhibitor. Of the group with inhibitor (n=6): one patient received activated recombinant FVII, while the others received FEIBA (mainly non-activated factors II, IX and X, as well as activated factor VII)".
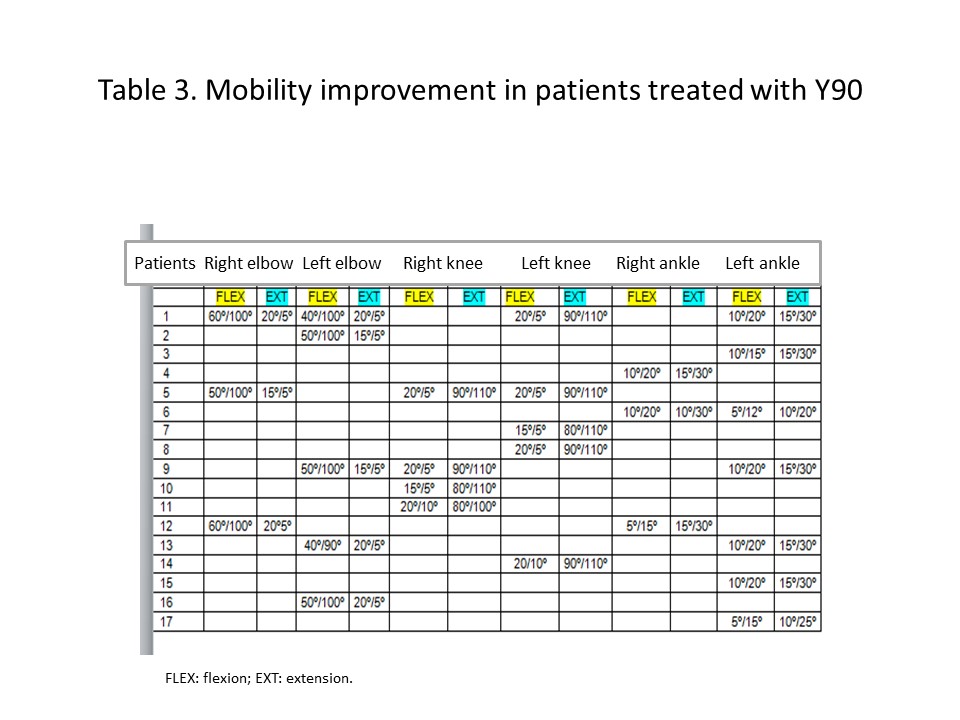
After the application of C-Y(90), a cotton bandage (called Jones' bandage) was placed for three days, and rest with limb elevation at home was indicated; ambulation was allowed in those who presented hemophilia type A and B without inhibitor. The response to the procedure was evaluated by the presence / absence of bleeding of the treated joint, with monthly assessment, and then every three and six months during the follow-up time before being discharged from the Pediatric Unit.
Patients with inhibitor were admitted to the hospital for two or three days to administer the necessary medication and to control bleeding. Depending on the affected joint, the procedure, type of hemophilia, and its severity, substitution therapy was maintained.
{kind=link}
{kind=link}