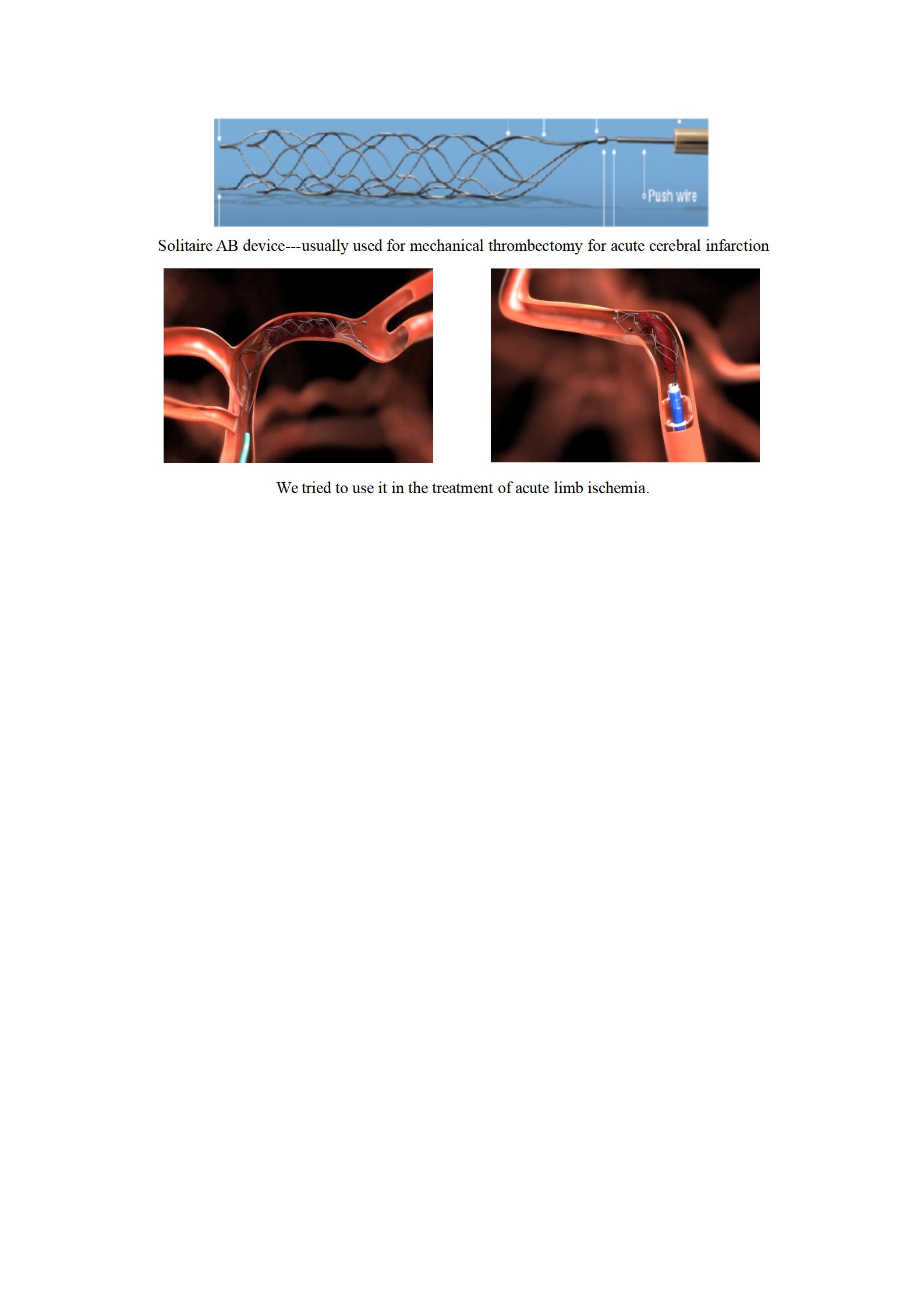
ALI is one of the most common acute and critical diseases with a high incidence, which has rapid progression.Without timely treatment, it will develop into ischemic necrosis with irreversible limb necrosis as well as significantly increased mortality. Early detection, diagnosis, and treatment are key factors that can improve the prognosis of ALI patients[5]. The restoration of blood flow to an ischemic vascular bed, that is, reperfusion, is a major therapeutic objective after ischemia of an organ or tissue, which can save limbs that are on the verge of ischemic necrosis, and reduce the disability and mortality in the later period. In 1963, Fogarty advocated the use of balloon catheter embolectomy for limb arterial embolization, which achieved satisfactory results. Compared with open thrombectomy, it has the advantages of less trauma, good patient tolerance, and lower postoperative mortality. However, Fogarty catheter embolectomy also has certain limitations: (1) arterial incision is required, and the surgical trauma is relatively large; the endometrium of blood vessels is easy to be damaged, which may cause vascular dissection or recurrent thrombo-occlusion. (2) The distal small arteries and branch vessels that cannot be reached by the balloon catheter often have residual thrombus after operation, resulting in a higher postoperative amputation rate. (3) Lack of guidance under X-ray perspective, and the removal of the plug has some blindness. CDT has become a first-line treatment option for acute limb ischemia[6, 7]. It is currently mainly used for patients with SVS / ISCVS Rutherford classification I, IIA, and IIB who have no thrombolytic contraindications. Compared with open surgery, it has less trauma and technical difficulties can be evaluated by dynamic angiography to evaluate the effect, the advantages of less vascular endothelial damage, less reperfusion injury, dissolving thrombus, and exposing potential stenosis of the artery at the same time. However, CDT also has certain limitations. Its progressive recanalization of blood vessels can not quickly remove thrombus and restore blood flow perfusion[8]. For SVS / ISCVS Rutherford IIB patients, if blood supply cannot be restored quickly, there will be post-limb motor function impairment and the possibility of blood necrosis, amputation, or even death. Therefore, PMT came into being, which can achieve rapid volume reduction of thrombus to reduce the time of symptomatic lower limb ischemia. Some studies have recommended PMT as a first-line treatment for ALI[9]. PMT currently applied to peripheral blood vessels mainly includes:large-lumen catheter aspiration, hemolytic thrombectomy such as Hydrolyzer from Cordis, Oasis and Possis AngioJet from Boston Scientific, and mechanical thrombectomy such as Amplatz thrombectomy and Straub Rotarex. Many studies have confirmed the safety of mechanical thrombectomy for the rapid restoration of blood perfusion in ALI. Stent thrombectomy is different from the above PMT. Its purpose is to reduce thrombus load and rapidly restore the blood flow, which helps to improve the efficacy of thrombolytic therapy. The Solitaire AB is a laser-cut, self-expanding, and fully recapture able, split-design nitinol device which has been routinely used in mechanical thrombectomy for acute cerebral infarction. In addition to craniocerebral blood vessels, Solitaire AB stent has also been used to retrieve superior mesenteric artery embolism[10]. Studies have shown that for acute ischemic stroke, the vascular recanalization rate and prognosis of stent thrombectomy are significantly better than those of non-stent PMT in all PMT procedures[11].
In addition to the advantages of less trauma and simple operation, Solitaire AB stent thrombectomy also has the following advantages: (1) It can be directly released at the thrombus site to play a role of "tunnel", it can quickly open blood vessels to reconstruct blood flow, and improve the state of limb ischemia in the short term. (2) Its delivery system can achieve the distal arteries of the extremities, such as the dorsal foot arteries, plantar arteries, or palm arterial arches of the upper limbs to treat the emboli effectively. (3) It can be completely released and recovered many times. Repeated use can improve the thrombus clearance rate and reduce operating expenses.
We combined Solitaire AB stent removal with thrombus aspiration to reduce distal embolism and improve the recanalization rate. However, a distal embolism still occurred in the seventh case, which eventually led to amputation. Therefore, in later cases, a spider arterial umbrella device was pre-inserted before stent removal to avoid distal embolism.
Acute arterial embolism is mostly old cardiogenic thrombus or sclerotic plaque blocking the blood flow after shedding into the blood vessel which secondary to proximal or distal thrombus. Such emboli is not sensitive to thrombolytic agents. Solitaire AB stent thrombectomy has a good effect on fresh thrombi secondary to this type of emboli. The stent thrombectomy can completely remove the emboli and the secondary thrombus 24 h after the onset of the disease. Combining anticoagulation and arterial thrombolysis can completely dissolve the remaining thrombus in the blood vessel. However, the stent was originally designed for intracranial blood vessels. The diameter is only 4 mm and 6 mm, and the length is only 15, 20, and 30 mm. The friction between the blood vessel wall and the blood clot causes the blood clot to adhere to the wall of the stent to be retrieved. If the diameter of the embolized blood vessel is larger (> 6 mm), the use of the Solitaire stent to remove the embolus will be greatly weakened or even ineffective because the stent is not completely adhered to the wall.
This study has several limitations. First, this is a retrospective study of a single, two-year study of a small number of patients. Second, this study cannot evaluate the importance of stent removal and thrombus aspiration in this combined technique. Because this study is a small preliminary retrospective, the results should be interpreted with caution. Additional comparative studies are needed to determine the role of stent removal and thrombus aspiration in this combined technique.
{kind=link}