Study setting {9}
The study population will consist of the patients with known CF referring to the Cystic Fibrosis Clinic at Akbar Children's Hospital, Mashhad, Iran.
Eligibility criteria {10}
Inclusion Criteria
The inclusion criteria of the study are as follows: 1) one or more typical phenotypic features of CF and a minimum of an elevated sweat chloride concentration on two/more occasions or two mutations known to cause CF on separate alleles; 2) age of 5-18 years; 3) pulmonary and gastrointestinal involvement; 4) ability to perform spirometry maneuvers and the minimum FEV1 of ≥30% compared to the same age, gender, and height in the normal population; 5) the percentage of oxygen saturation based on pulse the oximetry of ≥90% at room temperature; 6) no cardiovascular, hepatic, and renal failure; 7) absence of celiac disease and rheumatoid arthritis; 8) no acute pulmonary exacerbation requiring hospitalization within the past four weeks; 9) absence of acute respiratory tract infection and 10) informed consent for participation.
Exclusion Criteria
The exclusion criteria of the study are the lack of adherence to the drug regimen and presence of drug intolerance like nausea or vomiting or any allergic reaction.
Who will take informed consent? {26a}
Initially, the objectives of the trial will be clarified by the main administrator to the children’s parents and legal guardians, and written informed consent will be obtained from them at the time of enrolment.
Additional consent provisions for collection and use of participant data and biological specimens {26b}
We do not need any additional consent provisions
Interventions
Explanation for the choice of comparators {6b}
The Patients with eligible criteria will be enrolled to the study.
Intervention description{11a}
The Patients with eligible criteria will be enrolled to the study. Thereafter, With the use of the stratified randomization procedure, participants will be divided into two groups according to disease severity (severe/mild-to-moderate) using spirometry with 40% FEV1 cutoff range. Following that, simple sampling method will be used to select the patients from each group to receive either Nano-curcumin drop or Nano-curcumin-like placebo drop. (Figure 1)
Nano-curcumin (Exir Nano Sina Drug Company, Iran) is prepared as Nano micelle in the form of 70 milligrams of drops in 1 cc, and the placebo with the same color, taste and odor.
To adjust the drug dose for different ages and considering that the maximum acceptable dose based with the most significant impact and minimum side-effects was 80 milligrams, the required amount will be obtained for each subject based on the ratio of the body surface area of the patients. The curcumin and placebo glasses will be labeled A and B by Exir Nano Sina company, respectively and made available to the patients through the double-blind design. The duration of the treatment period is three months.
Criteria for discontinuing or modifying allocated interventions {11b}
Although no special side effect has been reported until now, with any intervention related side effects we will stop the intervention and report it to the Ethics committee of Mashhad university of medical sciences (MUMS) for decision making.
Strategies to improve adherence to interventions {11c}
In order to control patients for taking curcumin and placebo, they will be followed-up by phone every month. curcumin and placebo will be given to the patients for one month and patients will be asked to bring the bottle of drug in their next visit for assessing their compliance and if anyone used less than 70% of drop, he or she will be excluded.
Relevant concomitant care permitted or prohibited during the trial {11d}
Concomitant intervention will be:
1-Pancratic Enzyme Replacement Therapy(PERT): All CF patients with pancreatic deficiency need PERT for enzyme replacement as a regard we enrolled CF patients with gastrointestinal involvement, all of our patients use Creon as a usual treatment that doses are adjusted to the level of dietary fat. 2-Antibiotic: Tobramycin inhalation is an antibiotic which is used for pseudomonas infection. 3-Anti-inflammatory: Low dose azithromycin treatment frequently prescribed chronically as an anti-inflammatory effect in CF patients six years and older. We use it in our patients. 4-Anti Acid: suggested for patient who fail to respond to maximal dose of PERT and in patient with reflux disease.
5-Inhaled hypertonic saline: nebulized hypertonic (7%)saline is recommended twice daily to all patients six years and older. We use it in our patients. 6-Inhaled Beta2 agonist: is administrated in CF patient with moderate to severe lung disease twice a week.
7-Fat soluble vitamins: for all CF patients with pancreatic deficiency.
Provisions for post-trial care {30}
Outcomes {12}
The primary outcomes of the current trial are changes from the baseline to three months of the intervention in the inflammation at three levels: systemic inflammation by assessing IL-6 as an inflammatory agent, IL-10 as an anti-inflammatory agent, and hs-CRP level in the blood samples, pulmonary inflammation with the neutrophil count, and bacterial/viral culture on the nasopharyngeal swab, and gastrointestinal inflammation with the calprotectin level in the fecal samples.
The secondary outcomes are changes in clinical assessment of the pulmonary symptoms via spirometry, anthropometric assessment stand on the BMI Z score, and evaluation of the quality of life using the CFQ from the baseline to three months of the intervention.
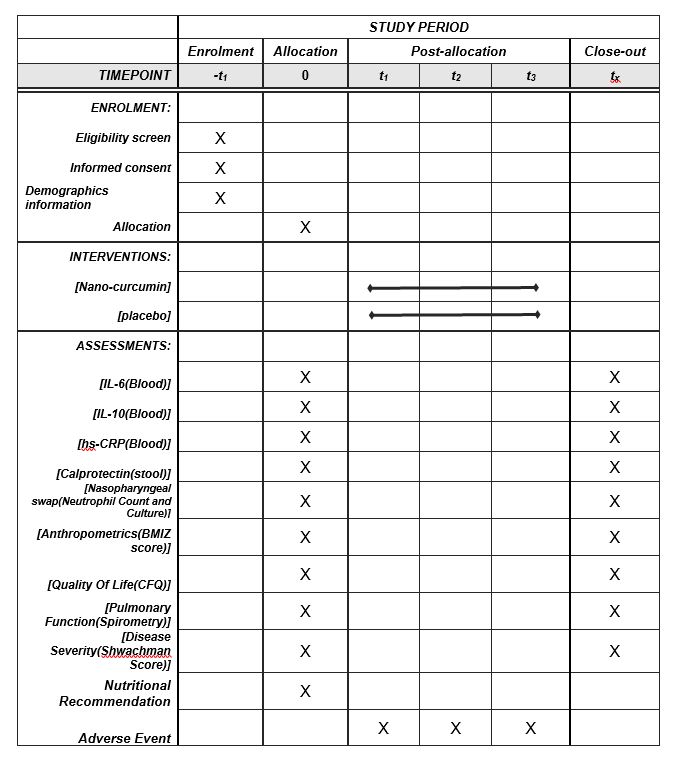
Participant timeline {13}
Nutritional recommendations will be provided to all the patients and/or their parents and legal guardians stand on the CF requirements and adjustable CREON dosing to the level of dietary fat. In addition, the patients and their parents completed the CFQ depend on age.
Anthropometric measurements (weight and height) will be performed using a digital scale (model: SECA). Body weight will be measured without shoes, and height will be measured in the standing position without shoes with the heels stuck to the wall and the head looking frontwards with the accuracy of 0.5 centimeter.
The fecal examination will be performed before and after the intervention. Before intervention, fecal sample will be evaluated for bacterial over growth and parasite specially giardia by checking stool PH and trophozoites or cysts of giardia. Any positive result will be treated with antibiotics before stating the trials.
Blood sampling will be performed before and after the intervention. Approximately five milliliters of blood will be collected, immediately centrifuged, the serum will be separated from the sediment, and preserved at the minimum of temperature of -20°C.
The primary and secondary consequences of the treatment will be investigated before and three months after the treatment. The clinical evaluation and follow-up of medication use and side-effects will also be carried out via phone call and paying monthly visit to the clinic, and the findings will privately be presented to the patients. (Table 2)
Sample size {14}
According to the lack of complete similar clinical trials which evaluate inflammatory effect of Nano-curcumin in children with cystic fibrosis, we used HSCRP indices as an effect size. Based on related article, the mean ± SD of hs-CRP indices in the curcumin and placebo groups, were 5.9(2.57) and 3.6(1.58). (16). G- power analyzer was applied for calculating sample size with a confidence interval of 95% and power of 80%. By considering 10% dropout and using Deff (deign effect) for stratified sample, a total of 30 samples for each group was calculated. In total, 60 eligible patients with CF are needed to include of randomization procedures.
Recruitment {15}
During regular monthly visit of patients at the cystic fibrosis clinic, treatment team specially nutritionist will explain the trial and discuss the advantages and disadvantages of therapy and answer any questions that participants may have.
Assignment of interventions: allocation
Sequence generation {16a}
The Patients with eligible criteria will be enrolled to the study. Thereafter, the first time with the use of the stratified randomization procedure, participants will be divided into two groups according to disease severity (severe/mild-to-moderate) using spirometry with 40% FEV1 cutoff range. The second time, simple sampling method will be used to select the patients from each group to receive either Nano-curcumin drop or Nano-curcumin-like placebo drop by using table of random numbers. (Figure 1)
Concealment mechanism {16b}
Table of random number is used to select patients from each group after stratified randomization based on disease severity. Also curcumin and placebo labelling is done by Exir Nano Sina company.
Implementation {16c}
Generate the allocation sequence, enrol participants, and assign participants to interventions will be done by the main administrative.
Assignment of interventions: Blinding
Who will be blinded {17a}
The curcumin and placebo glasses will be labeled A and B by Exir Nano Sina company, respectively and made available to the patients through the double-blind design in which neither the participant nor the experimenter are aware of which group.
Procedure for unblinding if needed {17b}
Data collection and management
Plans for assessment and collection of outcomes {18a}
Electronic registry form of cystic fibrosis in Khorasan province is an instrument for collecting the outcomes result.
Plans to promote participant retention and complete follow-up {18b}
In order to control patients for taking curcumin and placebo they will be followed-up by phone every month. curcumin and placebo will be given to the patients for one month and patients will be asked to bring the bottle of drug in their next visit for assessing their compliance and if anyone used less than 70% of drop, he or she will be excluded.
Data management {19}Research nurses and assistants collect the data at baseline and follow up and record it on electronic registry forms of cystic fibrosis in Khorasan province. Other additional date that is not available in the electronic registry form, will be recorded in the Excel file and in the paper forms at the same time. Also CFQ will be answered via electronic validated questioner by patients older than twelve years old. for patients younger than this age, clinical psychologist will ask them their questioner in the clinic.
Confidentiality {27}
Participants 'study information will be stored at the security site. All laboratory specimens, data collected, and reports will be identified by a coded ID number
Plans for collection, laboratory evaluation and storage of biological specimens for genetic or molecular analysis in this trial/future use {33}
We will try to collect a minimum two millilitre of blood sample for pharmaco-genetic and pharmaco-kinetic study in future use.
Statistical methods
Statistical methods for primary and secondary outcomes {20a}
Data analysis will be performed in SPSS version 20. The differences in the quantitative dependent variables will be evaluated using paired t-test or Wilcoxon test. The difference in the quantitative independent variables between two group, Mann-Whitney test or independent t test will be considered. The analysis of variance (ANOVA) or Kruskal-Wallis test will be applied for quantitative variable more than two groups. In all the statistical analyses, the P-value of ≤0.05 will be considered significant.
Interim analyses {21b}
Interim analysis is not considered. In case of frequent side effects (more than previous reports), we will stop the intervention and present the results to the Ethics Committee of Mashhad University of Medical Sciences (MUMS) for further decision
Methods for additional analyses (e.g. subgroup analyses) {20b}
Any covariates will be controlled by ANCOVA or binary logistic regression.
Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing data {20c}
For incomplete block of date's, we will use intention to treat analysis.
Plans to give access to the full protocol, participant level-data and statistical code {31c}
We will attempt to release the full study protocol and results as soon as possible, regardless of the magnitude or direction of effect. The anonymized data set and statistical code may be available from the corresponding author (Email: kianifar [email protected]) on reasonable request.
Oversight and monitoring
Composition of the coordinating center and trial steering committee {5d}
The ethical committee and vice chancellery of Mashhad University of Medical Sciences, supervises all the study stages. It is an academic committee and has no competing interest
Composition of the data monitoring committee, its role and reporting structure {21a}
We do not have a DMC
Adverse event reporting and harms {22}
Frequency and plans for auditing trial conduct {23}
Auditing trial conduct is not considered
Plans for communicating important protocol amendments to relevant parties (e.g. trial participants, ethical committees) {25}
Any modification to protocol which may impact on the conduct of the study, will be approved by ethical committee of MUMS prior to implementation.
Dissemination plans {31a}
We will attempt to release the full study protocol and results as soon as possible, regardless of the magnitude or direction of effect. The anonymized data set and statistical code may be available from the corresponding author (Email: kianifar [email protected]) on reasonable request.
{kind=link}