In this study, we found that family medicine physicians working in hospitals have higher rates of chronic disease management and higher rates of elderly patients than those working in clinics, and this discrepancy became larger in doctors younger than 40 years.
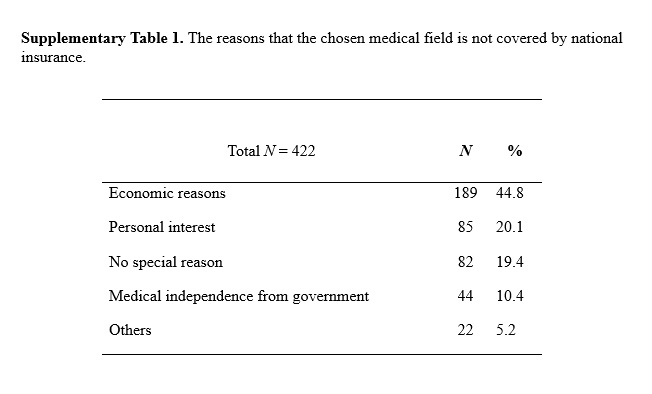
There are several possible reasons for the differences in medical treatment patterns of family medicine physicians between hospitals and clinics. Family medicine physicians in Korea have expanded to provide medical services not only for disease treatment but also health check-up centers, health promotion medical services, and new advanced medical technologies, which are classified as medical areas not covered by national insurance (7). As the proportion of total medical expenses classified as procedures not covered by national insurance has increased steadily in Korea, this phenomenon has also extended to family medicine physicians’ practice patterns (8,9). According to a report by the National Health Insurance Service (NHIS), medical expenses not covered by national insurance doubled during 2009 to 2014, and the proportion of noncovered health insurance expenses gradually increased from 13.4% in 2006 to 17.1% in 2014 (10). Moreover, the number of clinicians practicing only in noncovered medical areas in general medicine, plastic surgery, dentistry, and other fields has doubled in the last five years (9). It is recognized that the appearance-oriented culture that emphasizes measures such as anti-obesity treatments is one of the factors contributing to the demand for the various cosmetic procedures, including skin care treatments, plastic surgery, and anti-aging treatments (11,12). In this survey, 44.8% of family medicine physicians answered that the reasons for choosing a noncovered medical area are economic, 20.1% personal interest, and 10.4% to achieve independence from government restrictions on the right to medical treatment (Supplementary Table 1). There is a similar report concerning operating a clinic for economic reasons and the considerations affecting the choice of treatment area from the annual report of Korean Medical Association, which means that this phenomenon extends beyond family medicine physicians to other specialists who operate clinics (4).
Another reason for the changing medical practice patterns in young family medicine doctors is the instability of the medical delivery system, which has reduced the influence of primary medical institutions in the medical market share (13). The concept of primary care with a gatekeeper has not been established yet, and there are still many challenges to address before the possibility of each patient having his or her own primary physician becomes a reality in the Korean medical system (14,15). The number of family physicians who are newly entering the medical market has increased and clinicians, who are more vulnerable to the deterioration of the medical delivery system, may have been careful about incurring economic problems when choosing their primary care area, which is an issue more pressing for family medicine physicians working in clinics than in hospitals (13). For these reasons, we may assume that the trends in the medical treatment provided by young doctors are more likely to result in providing health promotion medical services than chronic disease management. More in-depth study of the differences in the tendencies of family medicine doctors working in clinics and hospitals are needed in the future.
This study also found that the number of days spent working days and nights were significantly higher for doctors working in clinics than in hospitals. This might be related to the operating hours of clinics and hospitals, and probably one of the reasons is that clinics usually open later and close later than hospitals. In addition, this factor is strongly affected by the medical treatment area and practice pattern in hospitals; for example, if a family medicine department in a hospital is oriented to outpatient medical care and health checkup centers, then there is no need for inpatient care and night duty work. In contrast, if a hospital is centered on hospice-palliative inpatient care, this requires more night duty work by family medicine doctors. A more detailed evaluation of working hours should be performed in the future for a more detailed assessment of doctors’ work environments.
The limitations of this study are as follows. First, the questionnaire survey is limited by subjective factors of respondents, possibly leading to under-reporting or over-reporting. Second, this study was conducted on the subjects who agreed with the usage of the personal information, and the limitation of the update of the group database in the society. Therefore, the representativeness of the samples was limited because our study was conducted in half of the total family physicians in Korea and the number of respondents was not enough.
Third, the study is limited by the lack of information on population samples covering the whole range of family medicine specialists and the standardization of the participants in terms of sex, age, and regional area. Nevertheless, this study is the first survey of family medicine specialists, as far as we know, that helps identify the medical practices of family medicine doctors and confirms the impact of decisions made during training on the medical care they will provide.
{kind=link}