Baseline characteristics – The baseline clinical and laboratory data of 340 included STEMI patients and four T-wave strata are described in Table 1. T wave amplitudes of ≥ 0, -1 to 0, -2 to -1, and < -2 mV were detected in 29 (8.5%), 153 (45%), 125 (36.8%), and 33 (9.7%) patients, respectively. Age was significantly different among groups (p-value, 0.001): patients with a T wave amplitude of ≥ 0 mV had the highest median of age (median [IQR], 70 [63, 78] years in patients with T wave amplitude of ≥ 0 mV vs 64 [54, 72], 56 [48, 67], and 55 [48, 59] years in those with T wave amplitudes of -1 to 0, -2 to -1, and < -2 mV, respectively). The majority of patients were male (82.9%). There were no significant gender-specific differences between four T wave strata (p-value, 0.136). The prevalence of diabetes and hypertension (HTN) was significantly different among groups (p values, 0.019 and 0.020, respectively) and they were more prevalent in patients with a T wave amplitude of ≥ 0 mV (34.5% and 51.7% in this group, respectively). Moreover, LVEF was significantly lower in patients with a T wave amplitude of ≥ 0 mV (median [IQR], 30 [25, 40]% in patients with T wave amplitude of ≥ 0 mV vs 40 [30, 45]%, 40 [35, 50]%, and 45 [40, 50]% in those with T wave amplitudes of -1 to 0, -2 to -1, and < -2 mV, respectively; p-value, 0.001).
Clinical outcomes – An overall, 62 patients (18.2%) developed VT/VF, and 24 patients (7%) died during the hospital stay. In-hospital mortality was higher in patients with a T wave amplitude of ≥ 0 mV compared to other T-wave groups (7 [24.1%] in patients with T wave amplitude of ≥ 0 mV vs 16 [10.4%], 1 [0.8%], and 0 [0%] in those with T wave amplitudes of -1 to 0, -2 to -1, and < -2 mV, respectively; p-value, 0.001, Table 1). However, no significant difference was observed between groups in terms of VT/VF rate (p-value, 0.801). Length of hospital stay was also significantly different among groups (p-value, 0.001) and patients with a T wave amplitude of ≥ 0 mV had significantly longer stay in hospital compared to other T-wave groups (median [IQR], 7.5 [7, 10] days in patients with T wave amplitude of ≥ 0 mV vs 6 [5, 7], 6 [5, 7], and 5 [5, 6] days in those with T wave amplitudes of -1 to 0, -2 to -1, and < -2 mV, respectively).
All the survived patients (316 cases) were successfully followed for six months. During this period, 70 patients (22.2%) were re-admitted to the hospital and 28 patients (8.8% of followed patients) died due to cardiovascular causes (total six months cardiovascular mortality, 52 cases [15.2%]). Both re-hospitalization and mortality were higher in those with a T wave amplitude of ≥ 0 mV (p-values, 0.001 and 0.002, respectively, Table 1).
Relative Risks for clinical outcomes – The relative risks (RR) for aVR lead T wave amplitude thresholds were calculated using the T-wave amplitude in aVR lead 0 to − 1 mV as the reference group since nearly half the population was in this group. As the T wave amplitude in aVR increased, there was a progressive increase in the risk of in-hospital mortality, re-hospitalization, and six months-cardiovascular mortality (Table 2, Fig. 1). Moreover, there was a significant correlation between GRACE score and T wave amplitude on aVR lead (correlation coefficient [β], 0.354, p-value < 0.001, Supplemental Fig. 3).
Determinants of T wave amplitude in aVR lead – The multivariate regression analysis identified three independent predictors of T wave amplitude in aVR lead including LVEF > 40% (β, -0.278; 95% CI, -0.477 to -0.079), age ≥ 60 years (β, 0.195; 95% CI, 0.025 to 0.365), HR ≥ 90 (β, 0.184; 95% CI, 0.006 to 0.362). Other variables with non-significant correlations with T wave amplitude are described in Supplemental Table 1. Associations between T wave amplitude in aVR lead determinants and their correlations with patients' clinical outcomes are depicted in Fig. 2.
Performance of T wave amplitude in aVR lead for prediction of the short and midterm clinical outcomes vs. GRACE score – T wave amplitude at the cutoff point of 0 mV had high specificity (> 90%), but low sensitivity (< 50%) for prediction of the endpoints (including 6- month cardiovascular mortality, in-hospital mortality, and re-hospitalization (Supplemental Table 2 and Table 3). On the other hand, T wave amplitude at the cutoff points of -1 mV and − 2 mV exhibited high sensitivity (> 90 %), but low specificity (< 60%) for the prediction of all study endpoints (Table 3). The cutoff point of -1 mV had the highest Youden’s index value for all study endpoints. The sensitivity and specificity of T wave amplitude at the cutoff point of -1 mV were 86.54% (95% CI, 74.21 to 94.41) and 52.43% (95% CI, 46.49 to 58.32) for cardiovascular mortality in six months, 95.83% (95% CI, 78.88 to 99.89) and 49.68% (95% CI, 44.04 to 55.33) for in-hospital mortality, and 67.14% (95% CI, 54.88 to 77.91) and 54.47% (48.02 to 60.81) for re-hospitalization, respectively (Table 3).
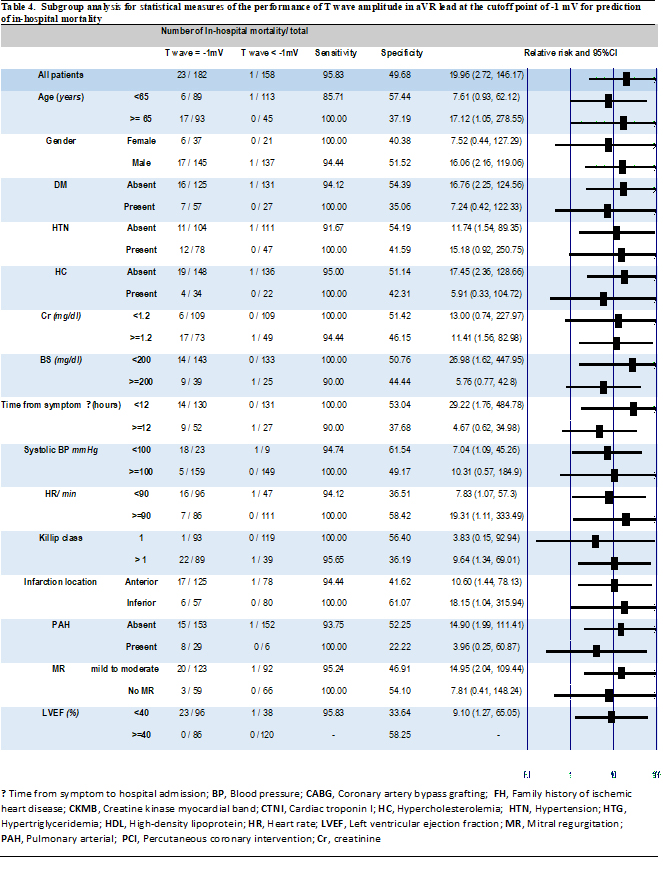
Nevertheless, subgroup analysis demonstrated that T wave amplitude at the cutoff point of -1 mV had higher specificity in those patients with better clinical conditions (age < 65 years, non-diabetic, non-hypertensive, with Cr < 1.2 mg/dl, early presentation [time from symptom to hospital < 12 hours, Killip class = 1, or having no PAH or MR, Table 4).
GRACE score indicated higher discriminative potential of prognosis toward the study endpoints (Supplemental Fig. 4). It had an AUC of 0.928 (95% CI, 0.883–0.973) for in-hospital mortality (optimal cutoff point, 167 with sensitivity and specificity of 83.3% and 83.7%, respectively), 0.935 (95% CI, 0.906–0.963) for six month-cardiovascular mortality (optimal cutoff point, 141 with sensitivity and specificity of 90.4% and 93.0%, respectively), and 0.757 (95% CI, 0.688–0.826) for re-hospitalization (optimal cutoff point, 149 with sensitivity and specificity of 50.0% and 93.3%, respectively).
{kind=link}