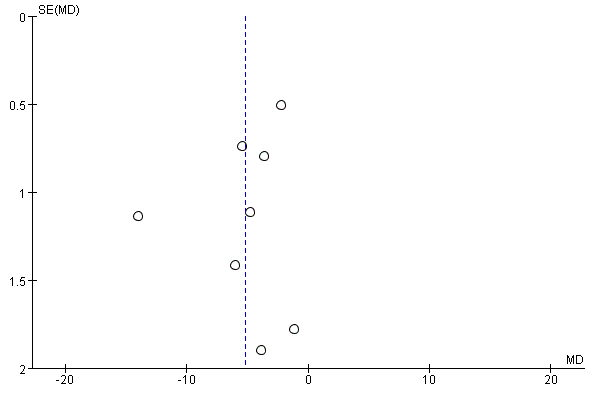
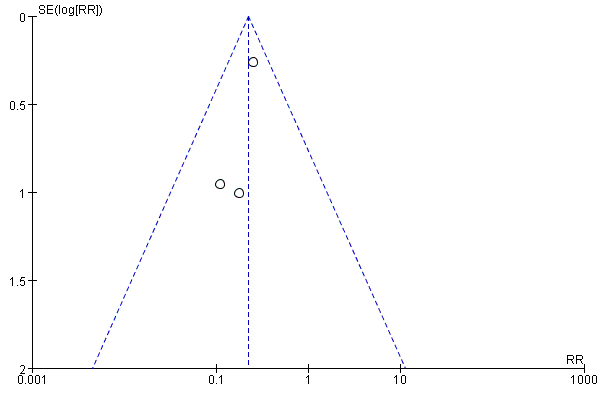
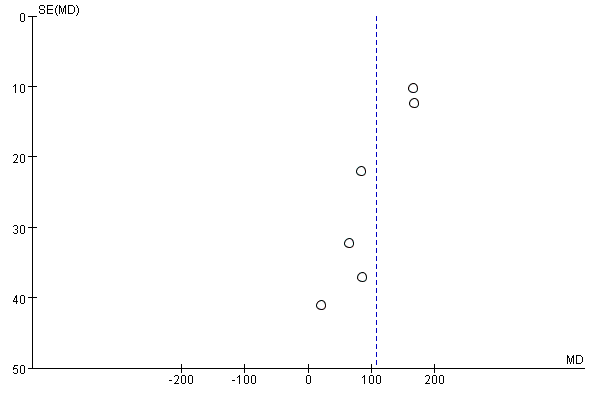
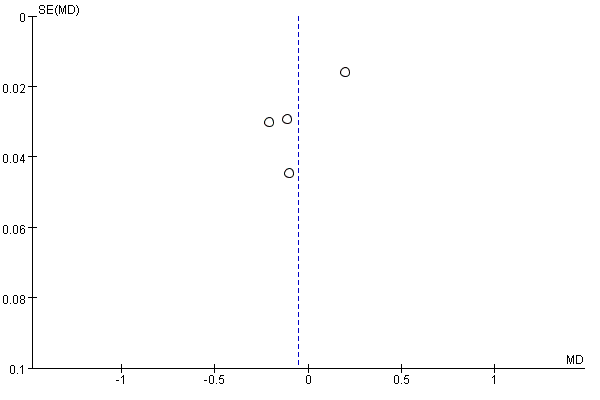
To our knowledge, this is the first meta-analysis to evaluate the effect of PADN on PH. We included a total of 8 PADN clinical studies including 213 patients with PADN. The results showed that after PADN, mPAP and PVR of patients were reduced, CO was significantly increased, but RV Tei index had no obvious changes. 6MWD and cardiac function of PH patients was significantly improved after PADN.
PH is a pulmonary vascular disease with complicated etiology and various treatment methods. There are a number of studies indicating sympathetic excitement involvement in the pathogenesis of PAH models and patients, so PADN targeting SNS could be a therapeutic strategy for PAH and right heart failure. The earliest animal experiment proved that PADN treatment could completely eliminate PH caused by balloon occlusion of the left pulmonary artery interlobar artery [23]. In dog, porcine and canine PH model, PADN improved the hemodynamics and alleviated right ventricular (RV) dysfunction [24, 25]. There were ablation damages to the blood vessels in the ablation zone, including intimal damage, thrombosis, elastic fiber damage and the reduction of the thickness of middle layer of blood vessel wall in porcine model [25]. In canine model, compared with the sham operation group, the thickness of the vascular wall and the pulmonary muscularization rate decreased in the surgical group, and the pulmonary artery remodeling was significantly improved [26]. Besides, PADN could inhibited the messenger ribonucleic acid expression of genes correlated with inflammation, proliferation, and vasoconstriction [26]. Huang et al. also proved that serum interleukins IL-1β, IL-6 and malondialdehyde levels in the PADN group were significantly lower than those in the sham operation group, and the activity of superoxide dismutase was significantly increased, suggesting that PADN may inhibit lung tissue inflammation and oxidative stress reduces PAH[27]. The above animal studies proved that PADN could improve PH hemodynamic parameters, and significantly improved vascular remodeling, reduced RV dysfunction and inflammation, but also caused vascular damage, which provided a basis for the clinical application of PADN. This study uses the basic principles and methods of evidence-based medicine to comprehensively analyze the published clinical studies on the PH of PADN. This study found that PADN could effectively improve the hemodynamic parameters of PH patients. However, the heterogeneity of these studies is high, and the source of the heterogeneity may be due to the difference in follow-up time, the types of PH and the use of targeted drugs after PADN of each study.
Some studies have reported that sympathetic nerve regeneration could occur in animal models with PADN, which might be related to sympathetic axon growth mediated by nerve growth factor secreted by abnormally proliferating pulmonary artery smooth muscle cells [26, 28]. Therefore, whether the effect of PADN decays with time deserves further study. Chen et al. showed that all variables of right heart catheterization and 6MWD improved significantly at 6-month follow-up and were nonsignificant different between 6-month and 1-year [17]. Current clinical studies have been followed up for up to 1 year, and no effect of PADN has been found to decrease with time [13, 17]. Therefore, we selected the data of 6 months and the closest follow-up time for 6 months for meta-analysis. 6-month follow-up studies conducted a subgroup analysis and found that the heterogeneity of mPAP, PVR and CO was significantly reduced, which indicated that differences in follow-up time might be one of the sources of heterogeneity
The use of PH-targeted drugs after PADN may also affect outcome indicators, but the studies we included involve both postoperative use and unused PAH targeted drugs. Various studies have shown that regardless of whether PAH targeted drugs are used after surgery, PADN can significantly improve the hemodynamic parameters and the life quality of PH patients. This meta-analysis also reached the same conclusion, but due to the unclear explanation of the postoperative medication history and insufficient research, no subgroup analysis was performed. As long as a reasonable control group is set up, the use of PAH targeted drugs after surgery will not affect the judgment of the efficacy of PADN.
Studies on PADN improving right heart function and which PH is more suitable for PADN are insufficient. Because RV function plays a critical role in the prognosis of PH patients, measuring RV function is essential to guide treatment and evaluate the progress of the disease [29, 30]. However, there is no accurate index to assess RV function. RV Tei index, tricuspid annular plane systolic excursion (TAPSE) and RV area change fraction (RVFAC) are currently the most commonly used methods for evaluating RV contractile function [31–34]. This meta-analysis found that PADN did not significantly change the Tei index of PH, which might be due to too little data Moreover, TAPSE and RVFAC are incomplete, so meta-analysis cannot be performed. In addition, global RV longitudinal peak systolic strain (RV-LS) is another indicator of right heart function, which is closely related to the clinical outcomes of PH patients, and is recommended as the preferred prognostic parameter [35–37]. Chen et al. reported for the first time the changes of RV function measures after PADN in Group I PAH patients and found that PADN could improve PH hemodynamic parameters, RV functional parameters and 6MWD, which were related to baseline RV-LS [18]. Specifically, baseline RV-LS ≥ − 11.3% might useful to predict which patients might benefit from PADN [18]. More clinical studies are required to assess the benefits of PADN in improving RV function and these parameters that reflect RV function should be valued.
In addition, Mechanisms, treatment methods and responses to treatment of different types of PH are different [38]. Apart from targeted drug therapy and etiological treatment, some patients with confirmed chronic thromboembolic pulmonary hypertension (CTEPH) can be cured by pulmonary artery endarterectomy (PAE) [39, 40]. PADN also could be used in in CTEPH patients with residual pulmonary hypertension after PEA [19]. And the research also proves that PADN has effects on many types of PAH such as connective tissue disease-related PAH, drug-related PAH, and idiopathic PAH [13]. However, due to the lack of current clinical research, most of the types of PH are not separately counted, so we cannot analyze whether there are differential effects of PADN on various PH. Furthermore, PADN could reduce the inflammatory response of PH animal models, but current clinical studies have not compared whether there is a difference in inflammation indicators pre-and post-PADN.
Most studies did not observe the occurrence of surgery-related adverse events, such as pulmonary artery perforation and the formation of dissection aneurysm or acute thrombus [13, 16, 17, 20]. Zhang et al confirmed that compared with the sildenafil group, the improvement of mPAP and 6MWD in the PADN group was more obvious, and the clinical worsening was less frequent [22]. These results confirm the safety and effectiveness of PADN. Based on the meta-analysis of these clinical studies, we came to a conclusion that PADN was a promising new strategy for the treatment of PH.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}