Background of the study
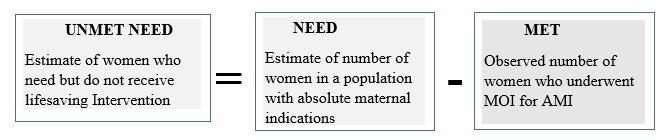
The concept of unmet obstetric need refers to the discrepancy between what the health care system should do to deal with the obstetric problem in a given population, and the care it actually delivers. Operationally, Unmet obstetric need is expressed in terms of women who should have benefited from an obstetric interventions, but for whom this intervention did not take place(1).
The unmet obstetric need network is the system that bring together ministers of health, development organization, scientific institution and practitioners who want to plan unmet need for major obstetric for absolute maternal indications as a starting point not just to improve maternal health but also the overall functioning of the health care system. The unmet obstetric need network provides technical support national teams involved in this kind of work, as well as opportunities to learn from each other(2).
The European commission and a number of other agencies decided to launch a formal UON network. The Unmet Obstetric Need Network brought together ministries of health, development organizations, scientific institutions and practitioners who wanted to map unmet need for “major obstetric interventions for absolute maternal indications” as a straight point to improve maternal health care and the overall functioning of their health care system(1).
The unmet obstetric need concept developed by the unmet obstetric need network considers unmet need by including major obstetric interventions that are done for absolute maternal indications and the gap between those expected and those actually done(2,3).
The discrepancy between the expected and observed major obstetric intervention rate for Absolute Maternal Indications, including CS, hysterectomy and destructive operations, is a powerful indicator of the unmet need for life saving obstetric care(4). The concept elaborated as: (See Concept in Supplementary Files)
Operational expression of the unmet obstetric needs concept adopted from previous study
The obstetric need is expressed in terms of the health problems, which necessitate an intervention, by the health care system. Among indications for intervention some are more essential to the survival of the mother and the child and others. These are called “absolute maternal indications (AMI) “; and it is on this basis that the indicator of obstetric is constructed. It is necessary, if the indicator is confined to major obstetric interventions for absolute maternal indications (MOI/AMI), in a way that is most relevant to the planning of the minimum interventions required. The AMI are severe ante partum hemorrhages caused by the placenta praevia or a retro placental hematoma (premature detachment of a normally inserted placenta), incoercible post- partum hemorrhages, major foeto-pelvic disproportions (due to narrow pelvis or a hydrocephaly), transverse positions (shoulders neglected) and face presentation(5,6).
The major obstetric interventions for absolute maternal indications comprises caesarean section, laparotomies, hysterectomies, internal versions, craniotomies or embryotomies and Symphysiotomy which may be carried out to avoid a caesarean in a case of Cephalo-pelvic disproportion(7).
Globally, 289, 000 women died from pregnancy related complications in 2015(9), half of them due to hemorrhage, hypertensive disorders and sepsis(19).
Number of facilities with emergency obstetric service is an important indicator. According to UN recommendations, there should be at least one comprehensive and four basic EmOC facilities per 500,000 populations. An estimated 15% of pregnant women develop major direct obstetric complications that require medical care, so the recommendation is that at least 15% births should take place in EmOC. This estimated through the met obstetric need which is an indicator for the interventions conducted for those with AMI should be 100% with the expectation that all women in need of major intervention get it from the health system(8,20).
The Unmet Obstetric Need assessment in five African countries, Benin, Burkina Faso, Mali and Niger shows that the percentage of deliveries receiving surgery for Absolute Maternal Indications was 1.4% in urban areas with functioning hospitals(22) the UON network states, 1.4% was practical low end estimate of the proportion of deliveries that require MOI to avoid maternal death(3).
A survey conducted in seven poor African countries only 1.1% of urban and 0.3% of rural mothers actually benefited from major obstetric interventions. In other word the deficit if unmet obstetric need was 25% in urban and 79% in rural areas(2).
Study conducted to assess UON in Zambia, revealed that unmet obstetric need was 41%. The rural population that suffered the entire deficit, was 73% implying that 77 out of 106 women and unmet needs in 2010. Further, the likelihood of undergoing a major obstetric intervention was 5.5 times higher in women from urban compared to rural areas, which underscores the unacceptably large inequity between urban and rural societies. The substantial rural-urban disparity demonstrated in the present analysis of unmet obstetric needs should alert policy makers and the health care system to improve lifesaving services to rural areas. The commonest indication for major obstetric intervention was Cephalo-pelvic disproportion(13).
Post-operative complications significantly dropped between 2008 and 2012 among patients presenting with non-AMI (P=0.008). No significant change was observed in patient AMI. The most frequent AMI were CPD 71% versus 70%, followed by uterine rupture and pre-rupture. Previous C/S was the main non AMI in 2008 (35%) and 2012 (37%)(23)
Retrospective assessment of UON in Dawro zone, 585 of mother with life threatening was obstetric complications was unable to get intervention and this was interpreted as the number of women who should have helped from a lifesaving intervention but actually did not. Major obstetric interventions for AMI rate of 0.8% and caesarean section took the largest share (81.5%) and the commonest AMI was obstructed labor 39.5%(5).
Met need for EmONC in all facilities was below 50% in all regions even as low as 3% in Gambela, Somali and Diredawa and higher in Addis Ababa 83%. The fully functioning of comprehensive EmONC was 148% of the 184 recommended leaving a gap of 36 facilities. The least available facility was in SNNP and Diredawa (22%) and the greatest in Harari (126%) which exceeded the minimum recommended number of EmONC facilities while other regions were below the national average (40%)(24)
Among all maternal deaths, 43% were related to direct obstetric complications, 5% indirect causes and 52% were due to unknown or unspecified causes. In this assessment the leading known cause of death were PPH/retained placenta and APH together responsible for 12% of death and severe pre-eclampsia or eclampsia for 10%, more over 26% of maternal complications were due to other direct obstetric complications but responsible for 12% death(25).
A review of caesarean cases 74% were found to be maternal indications, 22% were due to foetal indications- i.e. foetal distress and mal presentation. Indication related to CPD, prolonged and obstructed labor and arrest disorder 39%, foetal distress and non-reassuring foetal heart rate 13% and previous scar 13% was the leading indication for CS. Elective CS were most common among women with a previous scar was 47%(24)
A cross-sectional study conducted in Zambia revealed that, Major obstetric intervention for AMI were higher in urban 2.1% than in rural areas 0.4%, with an urban to rural rate ratio of 5.5. (13)
There is an important gap regarding the availability of service in women living in areas classified as urban, and thus residing within 10km of the hospital, the 55 MOIs for AMI represents 0.9% of all deliveries and 183 MOIs for AMI in rural women represents 0.5% of all deliveries.(5)
Thus this study has an important contribution to determine the prevalence of unmet obstetric need and recommendation to decrease maternal mortality for decision maker among the selected community in North shoa Zone Amhara region, Ethiopia.
{kind=link}