Nanoparticles for over forty years have been the subject of a large number of physical and bioscience research.1 In the last decade use of these particles in medicine has gone from theoretical to clinical trials.2 Current biomedical research now suggests nanoparticles will in the near future provide cancer patients with targeted drug delivery, manipulation of cancer microenvironment, provide radiosensitization and chemosensitization, aid in immunotherapy, and are the basis for new methods in bioimaging. 3– 19.
These tiny particles get their name from their size, ranging from 1 nm to > 100 nm. Construction occurs at the molecular level using chemical interactions between different compounds and elements.19, 20, 21, 22 Based on their size, nanoparticles are, in fact, well matched to interact with biological molecules found inside and outside cells. For example, mammalian cells range in size from 2000 nm to 10,000 nm, cellular organelles are about 100 nm to 300 nm, and intracellular proteins and molecules range between 10 nm to 50 nm. 23
Nanoparticles have several attributes that support their use in biomedical research and medical therapy at a microscopic level. First is their large surface area to volume ratio, allowing significantly increased chemical reactions to occur on the surface of nanoparticles.19 A second property is that they are often an appropriate size for intravascular conveyance and targeted accumulation in tumors.19, 24, 25 These properties among many others give nanoparticles a potential to target and manipulate tissues at a molecular level.23
What compounds/elements used to make a nanoparticle define how they can employed in medical or cancer therapy and/or radiology.1– 3, 10, 19– 21 Nanoparticles are most often constructed using more than one compound, such as silicone and metals or lipids and glycols. Biologic behavior of a nanoparticle is dependent its molecular nature. Targeting of nanoparticles to specific tissues, such as cancer, is through active or passive mechanisms. 1– 3, 11, 19 For example, attaching ligand a to the surface of a nanoparticle will actively target it to specific cells through cell surface receptors interaction, such as transferrin or folate receptors. Nanoparticles can also be targeted by attaching monoclonal antibodies or small molecules. 1, 12, 24
Nanoparticles made of elements or metals, such as gold, can be used to enhance radiographic imaging or be used induced to vibration with exposure to appropriate wavelengths of light. Metal-based nanoparticles in combination with laser produced light are already in pilot studies or clinical trials. Early data on this combination suggests that it is possible to perform targeted heating of tumors; achieving both coagulation of tumor vasculature and heat induced apoptosis or necrosis. 1– 4, 6, 9, 14, 17, 19, 26, 29
Passive targeting of metal based nanoparticles takes advantage of inherent abnormalities in tumor vasculature (Fig. 1) allowing accumulation in solid tumors through a process known as the ‘‘enhanced permeability and retention’’ (EPR) effect.25 For example, a company in Houston, Texas created a gold and silicone nanoparticle (GSN) with a core of silicone and a shell of gold. Over the surface of the gold is an outer layer of polyethylene glycol (PEG).§ By including the PEG layer, GSN has an increased circulation time by reduced mononuclear phagocytic system clearance. 28 After passive accumulation in tumors, exposure of these tumors to a wavelength of near infrared light (808nm) causes resonance of gold atoms in the GSN shell. Reverberation of nanoparticles within the tumors causes conversion of light energy into heat energy.26
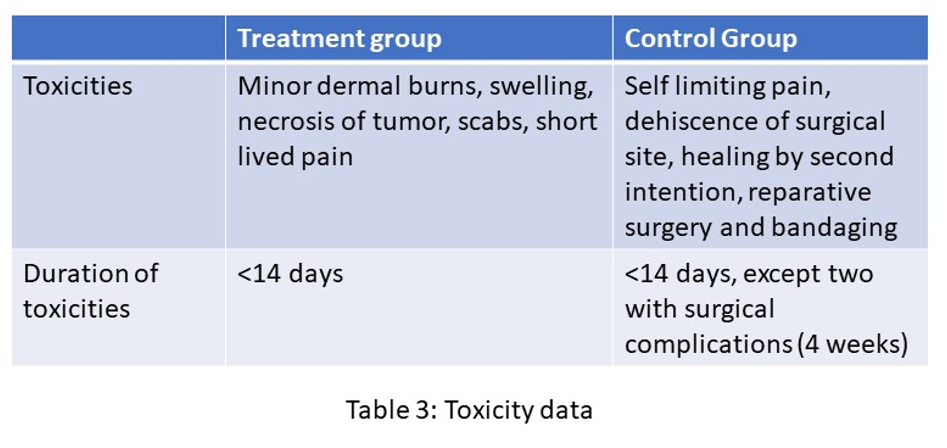
Previous research employing animal models has established that these inert GSNs are non-toxic, even at high doses. At a microscopic level there have been no toxicities noted in various organs, including the liver and spleen. The two organs responsible for clearing from circulation nanoshells not accumulated within tumors.27
In animal tumor implant models, combination of GSN and exposure of tumors to laser light (at 808nm) generated enough heat to cause tumor cell death.14 Near infrared radiance (NIR) has a low penetration into biological tissues. Thus, use of interstitial laser fibers are employed are required to achieve nanoparticle photothermal ablation for internal tumors. External light application will limit this therapy to superficial tumors/tissues.26
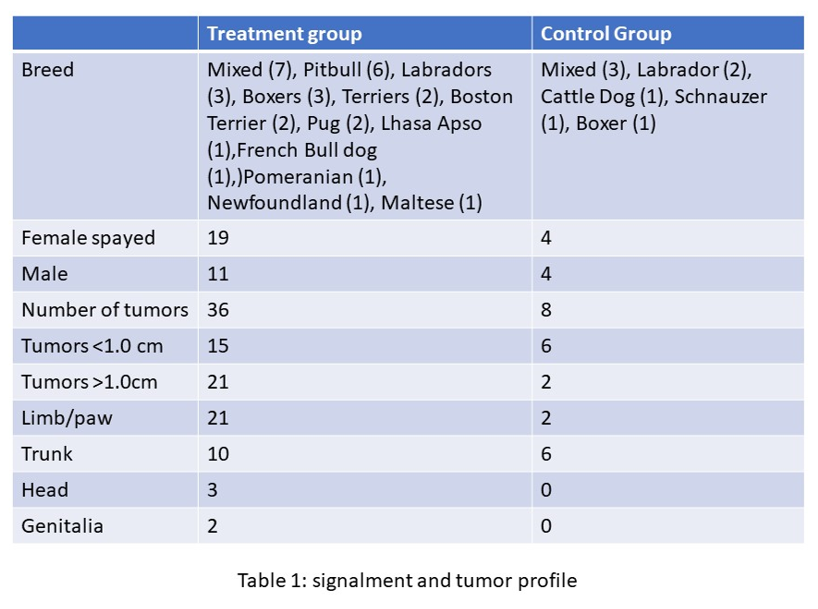
Based on initial pilot study data in various canine tumor types 4, ongoing human clinical trials in prostate cancer patients 31, and light-tissue interaction predictive modeling, low grade mast cell tumors were selected as our first spontaneous tumor model. Canine mast cell tumors are an excellent spontaneous tumor model in part due to their prevalence, a wealth of historical data, and a predominance of these tumors being dermal and subcutaneous. 33
Mast cell tumors (MCT) are the most common skin tumor in dogs, with an estimate of MCT being roughly 20% of canine skin tumors.31– 33, 39 Dogs may have solitary or multiple tumors at time of diagnosis, with dogs who form one tumor being more likely to form additional tumors .33 They can be located anywhere on the body but are most common in the dermis.31 – 33, 39 Genetically any breed can be affected but there are certain breeds predisposed to forming these tumors including Boston Terriers, Pitbull, Pugs, Labradors, and Boxers. 31 – 33, 39 A majority of MCT occur in the back half of the body with a large percentage of these affecting limbs, tails, and paws. All locations where complete surgical resection may not be possible without amputation or skin flaps.33
Prognostic factors for MCT in dogs are at times controversial. Factors that appear to impact long term control of the disease include location of the tumor, ability to perform adequate surgical removal, surgical margins, number of tumors at time of diagnosis, grade (both Kiupel and Patnaik grading schemes)36, 37, subcutaneous tumors, histologic pattern, multinucleation, Ki67, Ki67 + AgNOR, and KIT cellular localization pattern, and stage. Several of these prognostic factors have opposing reported data suggesting substantially different outcomes. For example, the controversy over impact of surgical margins and what defines an adequate margin. Unfortunately, no consensus has been reached on what recurrence rate can be expected for completely or incompletely resected tumors. In the literature recurrence rates range from 0–37.5% for clean margins and 12–63% for incompletely or narrowly resected (< 3mm) tumors. When factoring in grade, high grade (or high grade II or Grade III Patnaik) even with reasonable margins have a 40% recurrence rate.31–37, 39–44 It has been mostly accepted that grade of the tumor and surgical margins achieved during resection will impact long term tumor control.30– 37, 39, 40– 42
Regardless of the prognostic value of surgical margins, a majority of MCT can be cured or have long term control with suitable local therapy 30, 32, 33 Local therapies, other than surgery, are limited to radiation therapy (RTH) and electrochemotherapy.32, 33, 49 RTH has been suggested to reduce recurrence rates after incomplete surgical margins45 and may be able to act as sole local therapy.46, 47 Electrochemotherapy as an adjunctive treatment for incompletely resected MCT and as a sole local therapy has intriguing support in the literature.49, 50 Despite these two local therapies proven efficacy and durability of response, surgical resection is still considered standard of care for canine MCT.
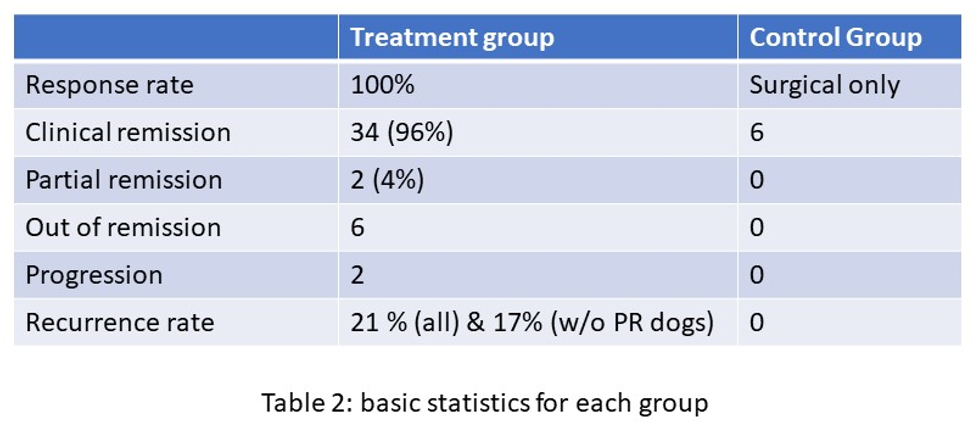
A pilot study testing nanoparticle and laser tumor thermal ablation on low grade canine MCT may provide an excellent opportunity to test PTA on a spontaneous tumor model and if PTA is successful the development of additional new local therapy against MCT. PTA may especially be found useful in MCT locations that are not amenable to achieving complete surgical removal. Our hypothesis in this pilot study is that photothermal ablation (PTA) using gold nanoparticles and near infrared light exposure will provide definitive therapy of low-grade mast cell tumors.
{kind=link}
{kind=link}
{kind=link}
{kind=link}