Study design
We conducted a cross-sectional, population-based study in December 2018 in 16 districts of southwestern Uganda. In this region, the local economy is largely dominated by subsistence agriculture, animal husbandry, and petty trading. Food and water insecurity are common (5,6). People aged 60 years and older comprise approximately 5% of the total population in the region (7).
Given our study’s focus on AD/RD, we sought to enroll people aged 60 years and older. Study participants were selected using a multi-stage area probability sampling of parishes. In the first stage, using a computerized random number generator, eight districts were selected from a list of 16 districts in southwestern Uganda. In the second stage, one sub-county (or an equivalent administrative local government) was randomly selected from an ordered list of all sub-counties in each of the 8 districts. In the third stage, one parish was randomly selected from each of the selected sub-counties. In each parish, we went door-to-door, recruiting participants consecutively using lists of older-age people that were provided by village health team members, until the required number per parish (50 people) was achieved. Upon approach, potential study participants were asked to confirm their date of birth by furnishing their national identity card. Participants were required to invite a consenting caregiver to answer questions about their activities of daily living. Participants did not need to be literate but were required to hear and see sufficiently well to communicate with study staff, answer survey questions, and undertake cognitive tests.
Survey instrument
We used the brief Community Screening Instrument for Dementia (CSID), which is suitable for use by non-specialists in low resource settings (8). The screening interview has two sections, with an interview for the person suspected of having dementia used to determine the CSID cognitive score (7 items; range, 0-9, higher score being better), and a separate informant section for a caregiver or close relation used to determine the CSID informant score (6 items; range, 0-6, higher score being worse). A CSID cognitive score £4 suggests probable dementia, a score of 5-6 suggests possible dementia, while a score ³7 suggests dementia is unlikely. For those with a CSID cognitive score of 5 or 6, we then interviewed the caregiver/informant. The inclusion of an informant interview is known to add to the validity of the brief CSID (8). The CSID informant score was subtracted from the CSID cognitive score to provide the total score (range, ‑6 to 9). A combined CSID total score (i.e., after subtraction of the informant score from the cognitive score) £4 is also suggestive of possible dementia. Thus, study participants may be classified as screening positive for probable dementia in one of two ways: (a) CSID cognitive score £4; or (b) CSID cognitive score 5-6 and CSID total score (cognitive score minus informant score) £4.
Following screening assessment for dementia, we administered a study questionnaire to elicit other variables, including vascular disease, lifestyle, psychosocial and psychological factors, infectious disease, and family history. Each variable was assessed by either being present (yes) or absent (no). Where necessary a family member provided further clarification during the interview. Study participants’ ages were cross-checked with their national identification cards and/or baptism cards. Formal education was defined as the number of years spent in school: none, 1-7 years (primary school), 8-11 years (ordinary level school), and 12 or more years (advanced level and tertiary education). Family history of dementia was elicited with a single self-report item identifying a first-degree relative (sibling or parents) who had ever showed signs of dementia or received a diagnosis of dementia. Lifetime history of cigarette smoking and alcohol were elicited using self-report. High-fat dietary intake was assessed with a single item eliciting a lifetime history of high-fat intake during the ages of 25-45 years, defined as regular, frequent consumption of animal products (e.g., milk, meat, ghee) or ground nuts. Religious integration was defined as participating in religious activities in addition to community prayer. To assess physical activity prior to 60 years of age, we asked a single question about heavy manual labor, riding a bicycle at least three days a week, or engaging in 30 minutes of exercise at least three times a week. Lifetime history of traumatic head injury was defined as ever experiencing head injury accompanied by loss of consciousness. We also elicited lifetime history of syphilis, tuberculosis, HIV, bacterial meningitis, cerebral malaria, type II diabetes mellitus, cerebrovascular accident, hypertension, epilepsy, limb paralysis, or thyroid condition. Study participants’ responses were cross-checked against any medical records kept in the study participants’ homes. An adequately ventilated kitchen was defined as one in which the household cooking took place in an open space or one in which there was ventilation from a window or chimney. All study tools were interviewer-administered in the local language (Runyankore-Rukiga). Survey questions were written in English, translated from English into Runyankore-Rukiga, and then back-translated to verify fidelity to the original wording.
Data management and analysis
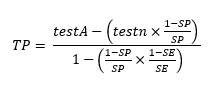
Data were entered, cleaned and analyzed using Epi Info version 7.2.2.6. As described above, the brief CSID provides an estimate of the screening prevalence of dementia. In most settings, the screening prevalence of dementia likely exceeds the true prevalence of dementia, due to the nonzero false positive rate. While the true prevalence of dementia is unknowable in the absence of data from a criterion standard (i.e., clinical diagnosis made on the basis of a structured clinical interview), we followed the “back estimation” method described by de Jager et al. (9) to estimate the prevalence of dementia based on our screening data and the known sensitivity (0.95) and specificity (0.90) of the brief CSID (8). First, we estimated the number of true positives given the well-known relationships between sensitivity/specificity and the number of test positives and test negatives: (see Equation 1 in the Supplementary Files)
We then used the estimated number of true positives to calculate the estimated prevalence rate.
We compared the proportions of those with probable dementia across different subgroups using the chi-square test. All variables with a statistically significant association with probable dementia on bivariate analysis were entered as potential covariates in a multivariable logistic regression model specifying probable dementia as the dependent variable.
Ethics approval and consent to participate
Ethical approval to conduct this study was obtained from the Mbarara University of Science and Technology Research Ethics Committee (reference number 13/10-18). Consistent with national guidelines, clearance for the study was granted by the Uganda National Council for Science and Technology (reference number SS 4842). We obtained administrative permission to enter the study communities from the district administrative head at each site. All study participants (informants and caregivers) provided written informed consent to participate. If a signature could not be obtained for literacy reasons, verbal informed consent was obtained in the presence of a witness and the study participant was permitted to indicate a signature using a thumbprint. For study participants who could not provide informed consent due to cognitive difficulties (e.g., presumed dementia), informed consent to participate was obtained from a caregiver, and the study participant was permitted to provide assent. All participants who screened positive dementia were referred to the nearest hospital (Mbarara Regional Referral Hospital, Kabale Regional Referral Hospital, Rugarama Hospital [Kabale], Kisiizi Hospital [Rukungiri], Nyakibale Hospital [Rukungiri], Itojo Hospital [Ntungamo], Kitagata General Hospital [Sheema], Kampala International University Teaching Hospital [Ishaka], or Ishaka Adventist Hospital [Ishaka]) for further clinical assessment and management.
{kind=link}