Using our algorithm, we have managed to distinguish the accumulation of 400-1,000 ml of air and fluid in the pleural cavity, from a healthy normal state, within twelve-second recordings while presenting high accuracy (64–100%, depending on the states examined), and regardless of background noise. When we tested the ability of the algorithm to predict PTX and/or HTX in each one of the various volumes combined, with no distinction between the different conditions and without pointing the exact volume - we obtained a high sensitivity rate of 81% alongside an accuracy of 80% in predicting the condition. The higher we increased the resolution of the test, i.e. answering, "Is there only PTX, of any volume between 400 ml and 1,000 ml?", without predicting the exact volume of PTX, we obtained a lower sensitivity rate of 63%, but with much higher specificity (94% compared to 69% in the previous calculation), with 80% accuracy. When we tested the algorithm at the highest resolution and attempted to classify the exact volume of the injury, in the range of 400 ml to 1,000 ml, accuracy dropped to 64% - a result which was expected, given the relatively small database and the complexity of the calculations. It is important to note that the algorithm fully identified HTX with 100% sensitivity, 100% specificity, and 100% prediction accuracy. However, we were unable to find a good predictor that could predict distinct volumes of HTX. Preliminary examination of the acoustic properties of the HTX samples exhibited a low signal-to-noise ratio, indicating a relatively high rate of background noise in comparison to the level of the desired signal. We believe this was due to the induction of HTX at the same physical location, shortly after draining out the air that was inserted earlier for the purpose of PTX induction. It is possible that some residual air remained in the pleural cavity, accentuating the presence of the injury beyond the increasing volume of saline. Nevertheless, it is important to note that we applied various computational methods, such as the Monte Carlo method, to evaluate the quality and the arbitrariness of the data and found it to be consistently balanced and protected from bias or overfitting effects. This means that the noise or random oscillations in the training set did not impair the predictability ability of the algorithm but rather result from the aforementioned cause. This also means that given more data, it is likely that we will be able to significantly increase the prediction accuracy. Although data describing morbidity and mortality of combat casualties exists from early conflicts in the 20th century, most of the modern knowledge and experience are based on US military operations in the Middle East, specifically in Iraq and Afghanistan. It is important to note that in relation to earlier conflicts, modern conflicts are characterized by an increased explosives utilization, such as improvised explosive devices (IEDs), grenades, and shoulder-fired missiles, resulting in higher rates of blast injuries and concomitant blunt thoracic injuries which are difficult and less intuitive to diagnose [26]. Israel Defense Forces (IDF) Medical Corps reviews conducted after Operation Protective Edge in 2014, also suggested tPTX to be one of the most common causes of preventable death on the battlefield, alongside hemorrhage and airway compromise [27]. A population-based study examining PTX incidence in severely traumatized patients in a civilian prehospital setting has shown that up to 20% of major trauma victims suffered from PTX with up to 15% of patients receiving emergency chest decompression [28]. Although considerable variation exists in the literature when addressing PTX size assessment, it is considered recommended to treat it when 30%-50% of the hemithorax (600-1,000 ml, respectively), is affected [29–31]. Considering the low clinical significance of a 200 ml PTX, and due to the technical issues described above, we decided to exclude those samples from calculations. The samples were recorded in the presence of mild background noise, and although its level was not measured, it can be inferred from the literature as the mean noise level in operating rooms is considered to be around 51–75 dB, as described by Hasfeldt et al. in their review [32]. Due to the limitations of in-vivo human experiments, the porcine model was chosen to demonstrate the feasibility, primarily due to its physiological and anatomical similarity to the human thorax. Previous studies described porcine pneumothorax models to be physiologically relevant to human extrapolation [33]. Future experiments should utilize the algorithm in human cadavers to construct human-based datasets.
A genetic algorithm was used to determine various parameters consisting the KNN algorithm and was also utilized in the process of creating the mathematical detector which identified the unique differentiating signature for each volume. Genetic algorithms are a family of optimization algorithms designed to streamline problem-solving by artificially activating a process that simulates the natural selection process underpinning the theory of evolution [34]. The method is based on applying small changes ("mutations") to randomly selected solutions for a certain problem, while producing new solutions and selecting those who better fit the target that has been defined by a “fitness” function and its stopping criteria; one would eventually achieve a near-perfect optimization within several runs (“generations”). This method is best used for solving problems for which the target is known but the way to attain it is unclear.
Among the aforementioned contemporary technological solutions for prehospital thoracic trauma detection, the most widespread modality is emergency ultrasonography. The E-FAST protocol may assist in assessing the presence of PTX and HTX, and to a lesser extent, its severity. Although the majority of studies present a very high specificity (> 95%) for the diagnosis of PTX in patients with thoracic trauma, they also exhibit a low sensitivity (~ 50%) when compared to other imaging modalities [35]. Prehospital emergency ultrasonography is noninvasive, portable, and inexpensive. Moreover, it has the advantage of being functional even in loud surroundings.
Nevertheless, it is heavily relied on provider experience and therefore may be time consuming, and it cannot differ acute HTX from chronic pleural effusions [36]. Although the latter may provide a challenge for our modality as well, we offer a non-provider-dependent rapid and objective detection modality, which may provide the actual volume of injury with higher sensitivity rate.
Diagnosing PTX using various acoustic techniques has previously been demonstrated in the literature. In their exploratory study, Mansy et al. demonstrated how the presence of PTX affects the transmission of sound waves across the thorax. During the study, which was conducted on 19 patients with iatrogenic PTX, a speaker was inserted into the endotracheal tube, and microphones were placed in various positions on the thorax. It was found that the presence of PTX affected the shape of the sound wave obtained when a 400-1,000 Hz signal was played when compared to a normal lung. Thus, suggesting a potential method for distinguishing between baseline and the presence of PTX [35]. Peng et al. presented a computational model simulating acoustic transmission from the lung to the thoracic surface in a porcine model under PTX. They found that introducing sound waves via the endotracheal tube may be measured by the transmitted waves from the thorax by a laser Doppler vibrometer [36]. A computational model of chest response to surface excitations via thoracic percussion was also presented by Peng et al. [37] thus presenting two potential methods for detecting pulmonary abnormalities, including PTX. A canine model for distinguishing PTX from baseline using vibrational response on the thorax following an external acoustic stimulation introduced via the endotracheal tube was described by Royston et al. [38]. Early studies describing the acoustic characteristics of breath sound suggested PTX cause amplitude reduction, decrease in high-frequency components, and reduced amplitude variation [39]. Hayashi introduced an external device that analyzed and converted the frequency of thoracic auscultatory sounds to numerical values and demonstrated how the presence of PTX could be detected with a sensitivity and specificity of 71.4% and 100%, respectively. His results were based on ten breath cycle recordings, which are equivalent to about 30–40 seconds. Confirmatory diagnosis of PTX was made by chest x-ray or a chest tomography and no data regarding the volume of the injury was provided [40].
In view of current literature, our method presents higher sensitivity and accuracy with shorter measurement times, regardless of background noise, and distinguishing PTX and HTX as small as 400 ml in volume. Moreover, our method utilized auscultatory data from a single spot on the thorax with no need for external excitation of any kind. Furthermore, while most studies refer to PTX diagnosis only, we managed to identify the presence of injected fluid in the pleural cavity, simulating HTX. Another clinical implication of our modality is that in the case of HTX, optimal resuscitation could be applied, and additional medication could be administered, such as tranexamic acid or fresh frozen plasma infusion. Moreover, chest tube positioning might be different if prior knowledge is available. In the case of PTX, one should point the tip of the tube upwards, while in the case of HTX, it should be pointed posteriorly and caudally. Due to rapid application of our modality, a near-instant follow-up could be applied, and patients treated with chest tubes could be monitored regardless of background noise. Equally important, proper use of our device can prevent unnecessary treatment in patients who do not require chest drainage.
 (TP-True positive, TN-True negative, FP-False positive, FN-False negative). In addition to comparing each of the volumes separately from each other, we conducted additional testing combining all observations with comparison to baseline (“volume 0”). A Pearson correlation coefficient was computed to assess the relationship between the real value and the predicted one. Calculations were made using a C# programming language in a LINQPad software utility.
(TP-True positive, TN-True negative, FP-False positive, FN-False negative). In addition to comparing each of the volumes separately from each other, we conducted additional testing combining all observations with comparison to baseline (“volume 0”). A Pearson correlation coefficient was computed to assess the relationship between the real value and the predicted one. Calculations were made using a C# programming language in a LINQPad software utility.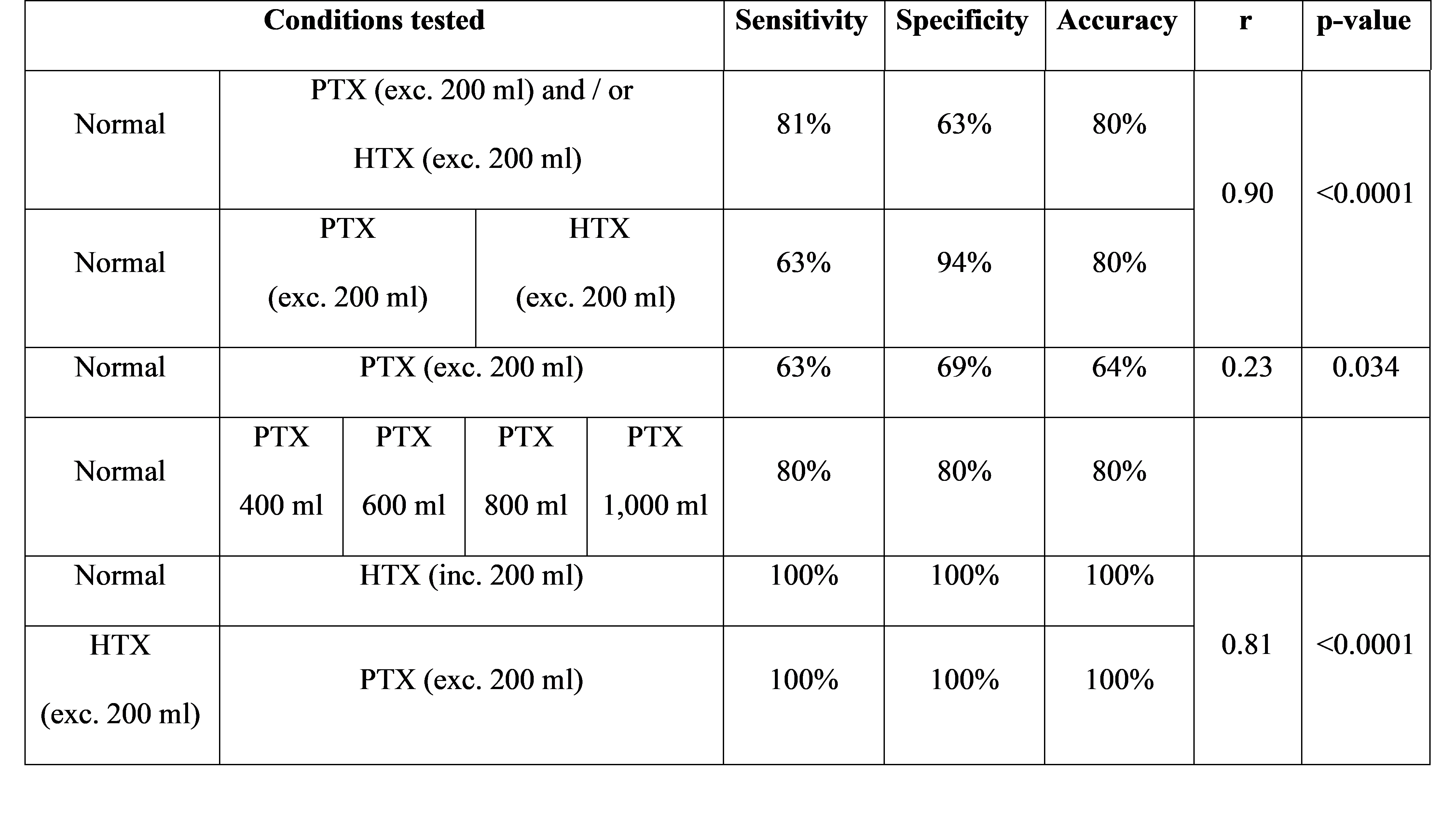{kind=link}