A prospective cohort study of all patients undergoing PRP or ESWT for PF was completed. The study was conducted over a period of 2 years from January 2015 to September 2016. The protocol was approved by the local ethics committee. All patients provided informed written consent prior to treatment and study participation.
Inclusion criteria: History of PF for more than 6 months; The obvious symptoms of plantar fascia (the patients have pain and swelling in the heel when they takes the first step in the morning or stays still for a long time); Evidence of PF on X radiographic and MRI examination; Signing informed consent and agree to review on time.
Exclusion criteria: Any previous local injection treatment for heel pain; Heel surgery history (Ankle fracture, talar fracture, calcaneal fracture, etc.); Foot deformity (flatfoot, clubfoot, tarsal coalition, etc.); Contraindications to this surgery included congenital collagen deficiency, BMI>30Kg/m2, severe heart disease, lesions affecting liver and kidney function, severe diabetes, central nervous system diseases, other medical diseases and pregnant or lactating women.
100 patients with plantar fasciitis were randomly divided into 2 groups (group A and group B) , 50 patients in each group. Patients were treated with autologous PRP injection in group A and with dolorclast radial ESWT in group B.
The group A (PRP):Twenty five of the 50 patients (50%) were male, and twenty-five (50%) were female. The average age for therapy was 48.8±11.3 (range, 33–70) years. Median follow-up duration was 28.2 (range, 24–35) months. The group B (ESWT): There were equal number of male and female patients in the B group:25 each. Average age was 44.9±9.6 (range, 32-68) years. The average follow-up time was 27.2 (range, 24–35) months. No differences were found between the demographic characteristics of the two different treatment groups (P> 0.05).
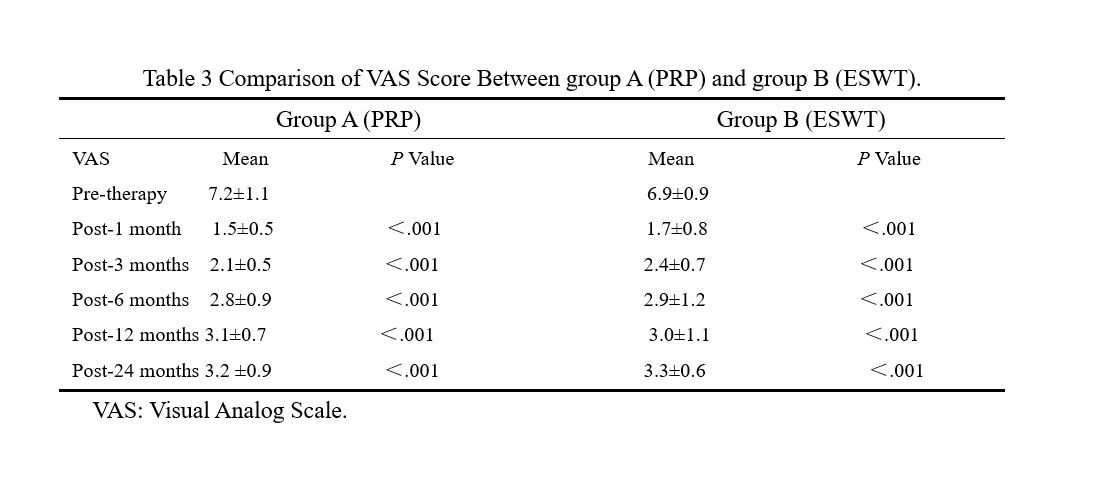
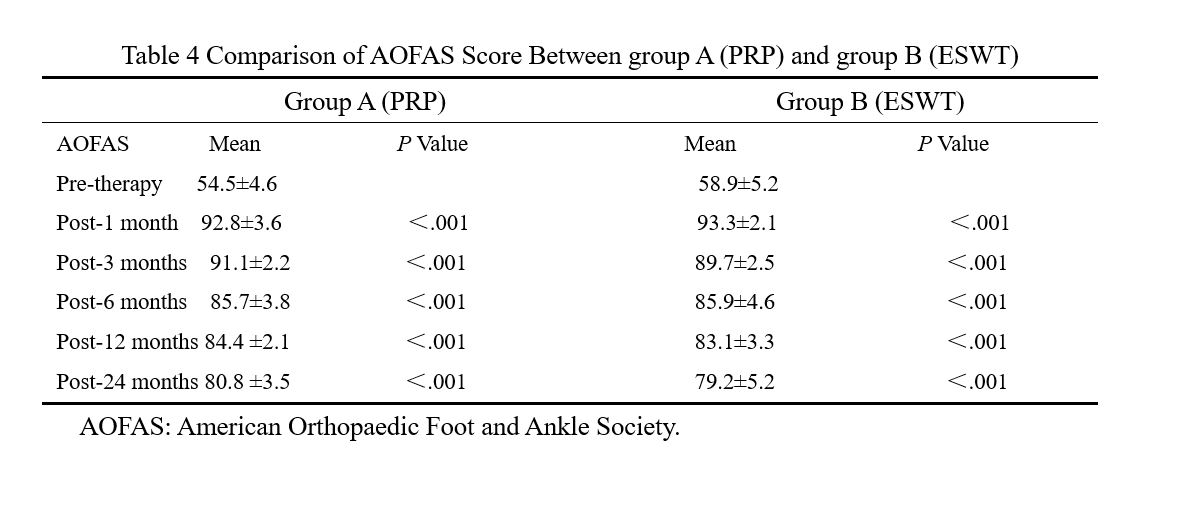
All patients were screened with plain radiographs and MRI to confirm the diagnosis of plantar fasciitis. Outcomes were assessed prior to the therapy and at 3, 6,12, and 24 months following the therapy, which included Orthopaedic Foot and Ankle Society (AOFAS) scores, visual analog scale (VAS) pain scores, subjective satisfaction score.
PRP:Under aseptic precautions, 27mL of the patient’s peripheral whole blood was obtained using an 18-gauge needle. Then, 3 mL ACD-A was added to the collected blood (in ratio of 1:9), and around 3 mL PRP was extracted by a double centrifugation technique at 1300 rpm for 10 minutes to separate erythrocytes and then again at 3500 rpm for 10 minutes to concentrate platelets using the Remi R-8C DX Laboratory Centrifuge (Remi Electrotechnik Ltd, Maharashtra, India).
The injection was given under strict aseptic precautions. The area to be injected was prepared with 10% povidone iodine scrub and draped with sterile towels. Injection was given by palpating the maximum tender point of heel with a medial approach with the patient in a prone position and ankle in a neutral position.
ESWT:Shockwave intervention was performed using an orthopedic dedicated divergent extracorporeal shock wave therapy machine (Switzerland, ENS). The patient takes a sitting position, and under non-anesthesia, according to the patient's pain point positioning (if the patient cannot be accurately positioned, it is positioned under the X-ray or B-ultrasound); the treatment site is determined, the coupling agent is applied to the treatment site, and the shock wave probe is placed at this time. position. Each impact is 2 000 times (8 Hz 2. 0 ~ 3. 0 bar), 7 days for 1 cycle, 4 to 8 times for 1 course of treatment; try to reduce strenuous exercise after treatment.
EFFICACY EVALUTION CRITERIA
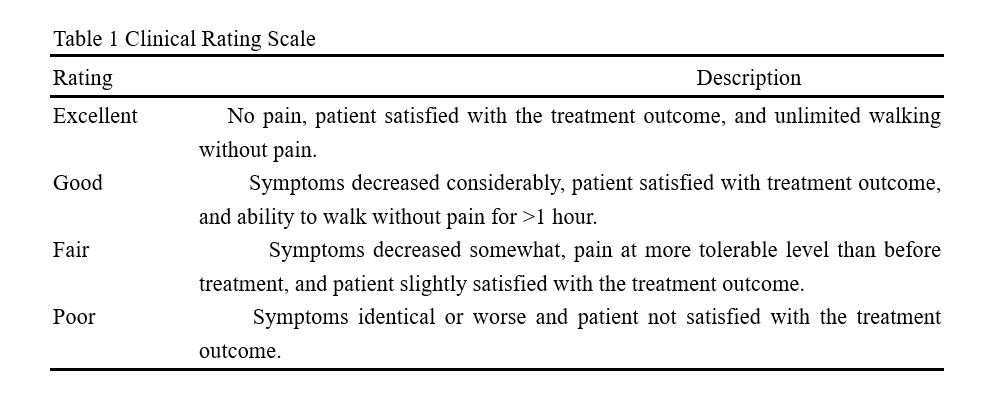
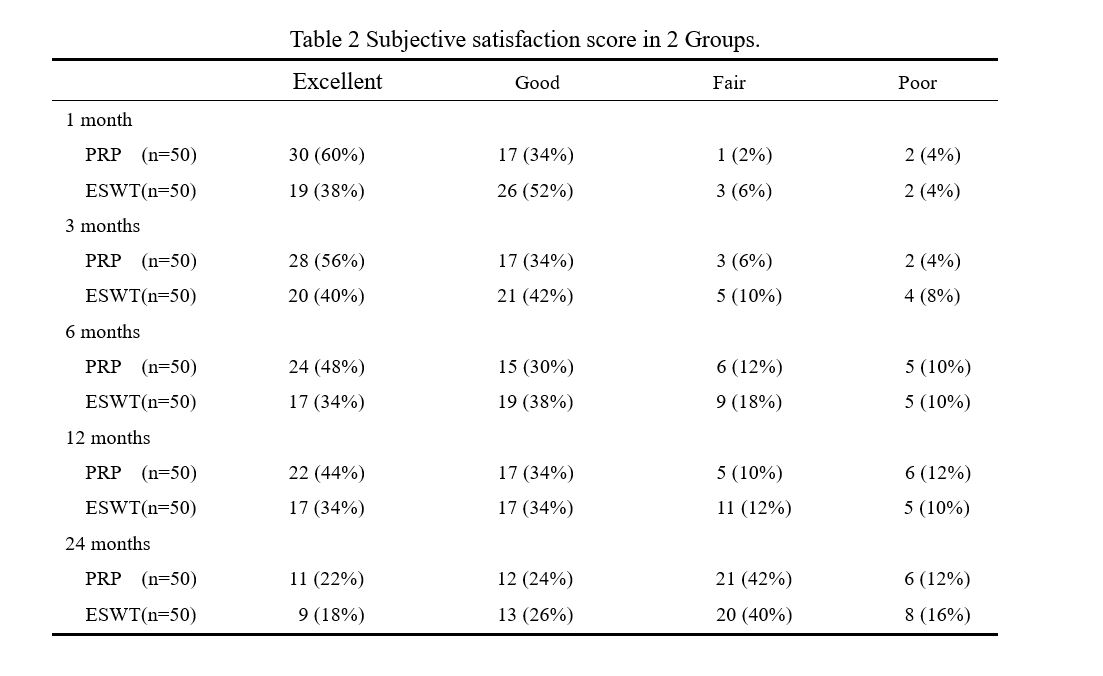
Patient satisfaction evaluation of treatment outcomes mainly includes ‘excellent’, ‘good’, ‘fair’, or ‘poor’. (Table 1) Outcomes were assessed prior to the therapy and at 3, 6,12, and 24 months following the therapy, which included Orthopaedic Foot and Ankle Society (AOFAS) scores, visual analog scale (VAS) pain scores and MRI studies.
STATISTICAL ANALYSIS
The statistical analysis was performed using the data analysis program SPSS Statistics version 16.0 software(SPSS Inc ,Chicago, Illinois, USA). Nonnormally distributed continuous variables were compared using the Kolmogorov–Smirnov test. For all statistical tests. The paired t-test and Wilcoxon’s signed-rank test were used to compare pre- and post-therapy values (AOFAS ankle-hindfoot scores, VAS scores, Karlsson ankle scores, and radiologic measurements). Statistical significance was accepted for P values<0.05.
{kind=link}
{kind=link}
{kind=link}
{kind=link}