Cancer is a significant public health problem and is the second leading cause of death globally13. Metabolic alterations of tumors are recognized as one of the hallmarks of cancer14. Cancer cells support energy to maintain tumor progression and proliferation by adopting to metabolic changes. A huge number of cancer cells show metabolic reprogramming, including the reprogrammed glucose, lipid and amino acid metabolism to satisfy high proliferation requests. FBG, ALB, TG and HDL-C can well reflect metabolic changes as routine clinical detection items, so they were included in this study. In addition, tumor cells need to survive drastic changes in the microenvironment such as hypoxia, nutrient storage, acidic pH and chronic inflammation15. The tumor microenvironment enforces metabolic plasticity and promotes tumor proliferation and progression16. Therefore, this study included PGSGA score as a sensitive to evaluate nutritional status, and included NLR as an inflammatory marker. Besides, we included some other indicators related to the survival and prognosis of tumor patients, such as age, smoking history, tumor stage and tumor metastasis, so as to more comprehensively predict the prognosis of cancer patients. There were also many indicators that can reflect tumor metabolism and microenvironment, but they were not included in this model due to the incomplete data, missing values>10%, being removed by stepwise regression and the results of multivariate analysis were meaningless.
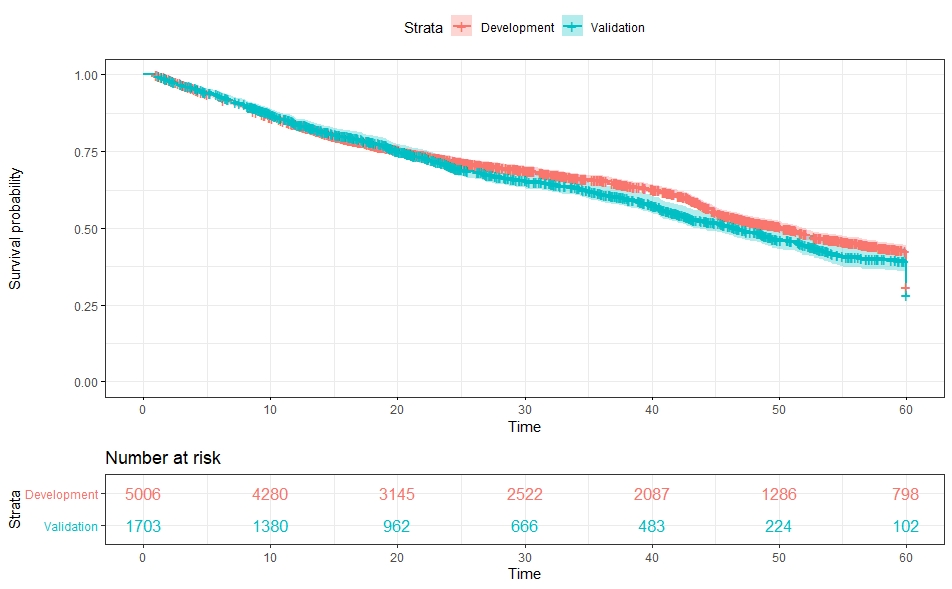
A clinical prediction model can provide tailored estimation on prognosis and help physician with associated decision making in daily practice. At present, many indicators of tumor metabolism are based on experimental metabolomics technologies, which cannot be widely popularized in clinical practice because of its high cost and long detection cycle. Therefore, we used routine clinical detection indicators in prediction model. In order to develop an accurate clinical prediction model, we conducted strict quality control. First, in order to build a reliable and accurate prediction model, the sample size should be large enough and the data should be complete. We screened from INSCOC database and included a large sample of 5006 in this study to ensure the quality of data development. Second, we ensured that the data covered common types of tumors, and all factors included in the prediction model are commonly assessed in routine clinical examinations. In this way, the universality of the prediction model can be guaranteed to the greatest extent and can be widely used in clinical practice, which is clearly a practical advantage. The model is available as a nomogram. Nomograms have emerged as a simpler, yet more advanced method to calculate the prognosis of different cancers. By integrating diverse prognostic and determinant variables to generate the probability of a clinical outcome, the nomogram fulfills a necessary role in oncological personalized medicine. In this study, the nomogram could predict an individual's 1-, 3- and 5-year survival rates with good accuracy which was verified in the validation cohort. This nomogram can evaluate the prognosis of patients conveniently and help clinicians adopt preventive and therapeutic strategies.
Normally, the main way for the body to obtain energy is the oxidative phosphorylation of glucose under aerobic conditions. In cancer cells, even in the presence of oxygen, the main pathway of glucose metabolism is aerobic glycolysis, termed Warburg effect4, which reflects the reprogramming of tumor glucose metabolism. Hyperglycemia is a common phenomenon in patients with advanced cancer17. Hyperglycemia can provide cancer cells with a high glucose fuel source to support rapid proliferation, drive glycolysis metabolic pathway, and lead to worse prognosis. Hyperglycemia can indirectly influence cancer cells through an increase in the levels of insulin/IGF-1, thus activating the PI3K/AKT/mTOR signaling pathway and promoting the development of cancer18. Beyond that, hyperglycemia has a direct impact on cancer cell proliferation, metastasis, invasiveness, and antiapoptotic qualities 19–21. In our study, FBG ≥ 6.1 mmol / L (HR 2.63, 95% CI 2.39-2.91) is considered as one of the risk factors affecting the survival of tumor patients, which confirms the harm of hyperglycemia. Hyperglycemia can promote glycolysis and raise the prevalence and mortality of certain malignancies. FBG is the most intuitive index to reflect blood glucose, which can be a prediction index for cancer progression and glucose metabolism 22–23.
Therefore, patients with FBG ≥ 6.1 mmol / L should be carried out appropriate diet or drug intervention to improve the prognosis.
In cancer cells, the protein synthesis and decomposition are enhanced, but the anabolism exceeds the catabolism, and can even capture the protein from normal tissues, in order to meet the needs of their own growth. The amino acid metabolism of the tumor was also changed, tumor cells can obtain energy through glutamine and other amino acids. These changes will lead to severe protein consumption, negative nitrogen balance and hypoproteinemia. Patients with hypoproteinemia have a greater risk of recurrence and mortality, which can be corrected by albumin supplementation. Albumin (Alb) is an acute phase protein that decreases with inflammation and due to other reasons, such as malnutrition, increased age and metabolic disorder. Albumin reflects nutritional state and response to amino acid metabolism, and is associated with the prognosis of cancer patients. In our study, ALB≥35 g/L (HR 0.71, 95%CI 0.63-0.80) was the protective factors of overall survival. Kao HK et al.24 showed that patients with increased serum albumin level can have better prognosis. Therefore, albumin can not only reflect amino acid metabolism, but also predict survival and prognosis as a biomarker 25–26.
Nowadays, there are increasing evidences of the role of lipid metabolism alterations as biomarkers of cancer prognosis and survival. Together with the Warburg effect and the increased glutaminolysis, lipid metabolism plays a key role in cancer metabolic reprogramming. Extremely proliferative cancer cells exhibit an intense lipid and cholesterol avidity, which they satisfy by increasing the uptake of dietary or exogenous lipids and lipoproteins27. In addition, the increase of de novo fatty acid synthesis and lipid synthesis in cancer cells requires efficient and complementary lipolytic mechanisms to accommodate the intracellular lipid content and provide materials for tumor cell proliferation28. This long-term metabolic change will lead to the depletion of stored fat, and promote cancer cell metastasis29. TG and HDL, as lipid indexes reflecting lipid metabolism, are closely related to prognosis. Studies showed that a high level of HDL-C can reduce the risk and progression of cancer30–31. In our study, HDL-C≥1.55 mmol/L (HR 0.65, 95%CI 0.59-0.72) were protective factor of survival. However, the association between TG and the survival of tumor patients is contradictory. Some studies observed that high level TG can improve the survival of cancer patients32–33. On the contrary, other studies30–34 has shown that high TG can lead to poor prognosis in cancer patients. In our study, TG≥1.7 mmol/L(HR 0.77, 95%CI 0.69-0.86) were protective factor of survival. Rhonda Arthur et al.35 showed that TG were not associated with cancer death, but associated with risk of cardiovascular death. This reduced the proportion of cancer cases of death in subjects with elevated TG levels. However, the detailed mechanisms and the biological significance of them require further investigation. In conclusion, Lipid-metabolic can associate with cancer survival and have been proposed as prognosis biomarkers of cancer36.
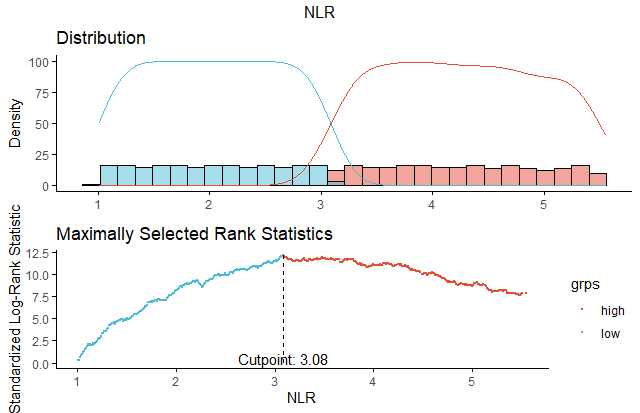
In our study, PGSGA score≥4(HR 1.46, 95%CI 1.32-1.61) and NLR≥3.08(HR 1.25, 95%CI 1.13-1.38) were the independent risk factors of overall survival. PGSGA score≥4 indicates the malnutrition in cancer patients, and these patients often have poor prognosis and low survival37. In this study, increased NLR was associated with decreased OS. NLR is the ratio of lymphocytes to neutrophils, the two types of cells are part of the human immune system and play a key role in TME. The immune cells in the TME can detect and eliminate the abnormal cells or tumor cells and protect the body from damage caused by tumor cells. Kao HK et al24. considered that an elevated NLR indicates an imbalance between the innate and acquired immune response, which might be linked to a poorer prognosis. This elevation may reflect an inflammatory microenvironment that lymphocytes can have tumor suppressing effects and have been linked with better prognosis38, whereas neutrophils can create a favorable tumor microenvironment by remodeling the extracellular matrix and angiogenesis, thus enabling the tumor to growth and spread39–40. Therefore, NLR can be used as a biological indicator of inflammation to predict the prognosis of cancer patients.
Some limitations of this study should be discussed when considering the results. First, cancer patients still have a lot of laboratory indicators reflecting the metabolic situation in clinic, so it is necessary to add more factors to improve the model in the future. In addition, although internal validation was performed to prevent over-interpreting the data, and external validation verify our findings are applicable in single center, we need a prospective multicenter study to confirm the results in the future.
{kind=link}
{kind=link}
{kind=link}