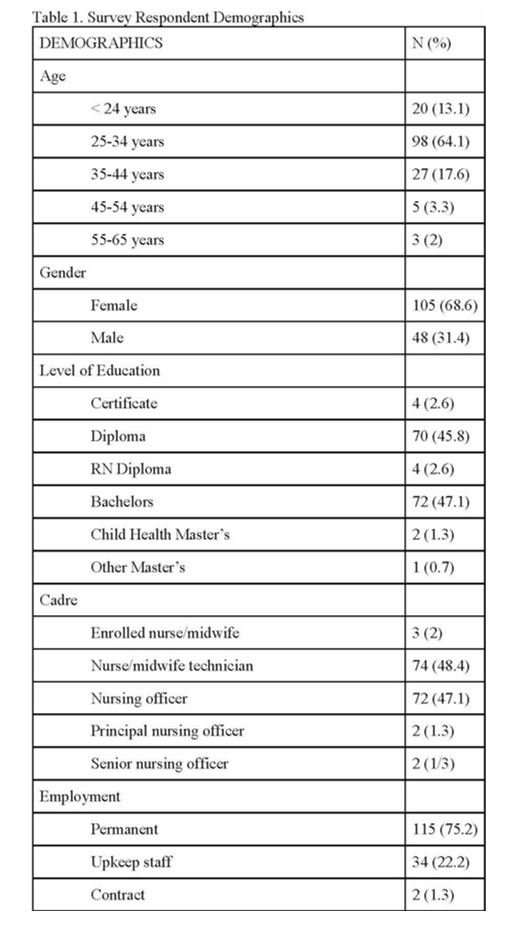
Needs assessments alone are not enough to impact patient health outcomes, so this study is the beginning of a larger education and practice change.[19] Nurses with master’s degrees have advanced nursing roles which enable them to provide clinical leadership, positively impact clinical practice, and improve the provision of care.[20] The findings indicate that only two participants were trained at the master’s level, and these are principal and senior nursing officers. As such, their primary focus is on managerial and administrative duties rather than to provide bedside nursing care. This calls for more nurses to be trained at the master’s level so that they can provide leadership in quality care of critically ill children.
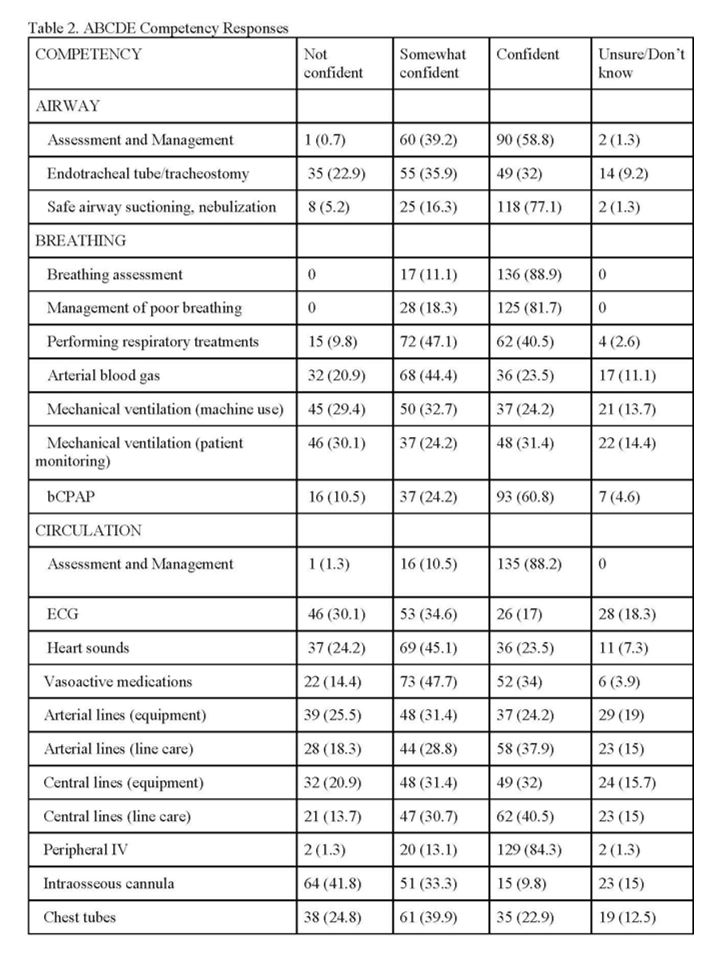
Overall, there were high rates of critical care confidence among nurses. For example, nearly all nurses felt confident or somewhat confident in assessment and management of skills across all ABCDE domains. A study in Uganda and Zambia showed that healthcare providers’ confidence increased with exposure to a variety of skills, which will be important to consider when designing the content of a PCC master’s program.[21]
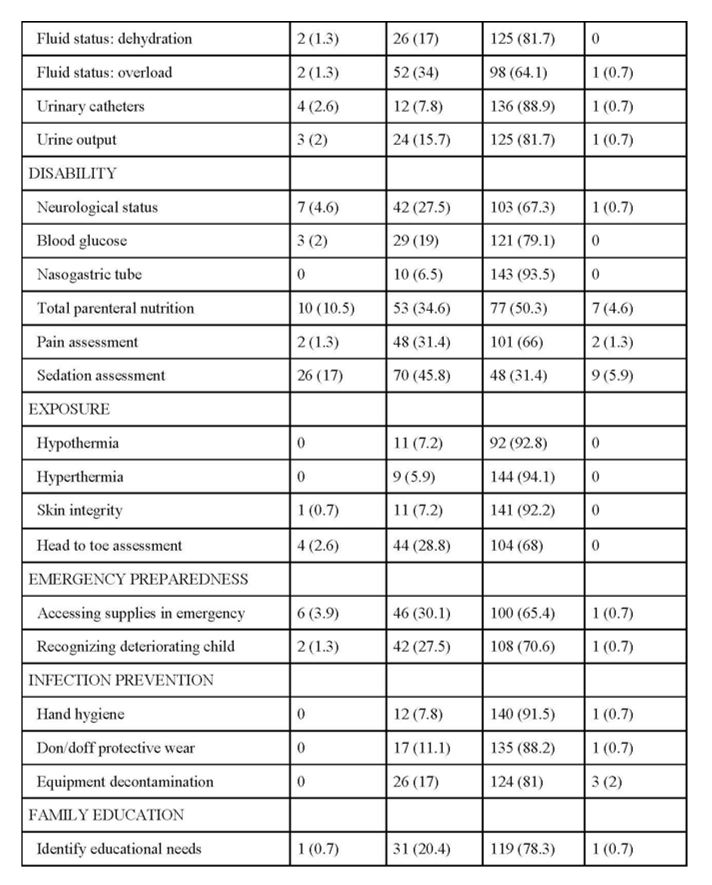
Nurses rated high confidence particularly in task-oriented or scale-dependent skills, including the Glasgow or Blantyre Coma Scale, blood glucose monitoring, nasogastric tube management, pain assessment, temperature monitoring, skin assessment, and infection prevention. Further investigation may be revealing as to whether nurses know how to interpret the data they collect, what intervention is indicated based on the findings, and when to reassess the patient, which would better demonstrate critical thinking skills and a higher level of nursing competency.[22]
Although nearly 97% of nurses indicated “confident” or “somewhat confident” to performing head-to-toe assessments and focused cardiac and pulmonary assessments, nurses indicated lower levels of confidence in listening to heart sounds specifically. This may indicate a gap in nursing knowledge, incomplete or rushed assessments, or a lack of understanding of how to interpret assessment findings. Comprehensive head-to-toe and focused assessments are more meaningful if nurses can interpret the findings, anticipate interventions, make recommendations, and monitor a patient’s response to the intervention because these actions help in identifying a patient whose condition is deteriorating. It will be important to identify the underlying cause of nurses’ lack of confidence as a matter of patient safety.[23, 24]
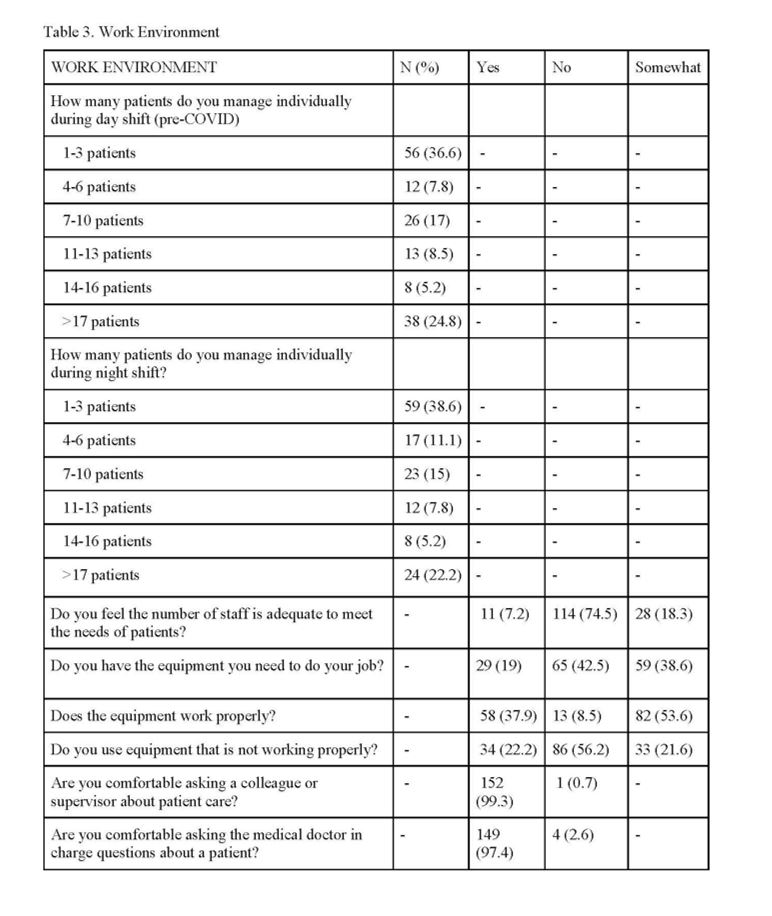
High patient volumes could affect the nurses’ ability to confidently perform assessments. Half the nurses care for 1–3 or 4–6 patients on a shift, which is comparable to some high-income settings such as California, USA, where state law requires a ratio of 1:2 for critical care wards and up to 1:6 in medical/surgical wards.[25] However, one third of nurses care for > 17 patients and 75–80% of nurses feel their ward is understaffed and underequipped. While almost 100% of nurses feel comfortable asking a colleague, supervisor, or medical doctor a question about their patient’s care, this still has great implications for the nurse’s ability to dedicate quality time to individual patients, provide thorough education, and quickly recognize clinical deterioration.[26] High patient workload in paediatric critical care settings is associated with long hospital stays and poor health outcomes for patients, and for nurses, increased medical errors and burn out.[26–28]
Findings highlighted other areas where most of the nurses were less confident. Half the nurses were not confident or somewhat confident in managing endotracheal tubes or tracheostomies, and a little over half of nurses were not confident or somewhat confident in managing mechanical ventilation. This was not a surprising finding as the only ventilators are located at PICU at MJC and in the main ICU at QECH, therefore very few nurses provide care for ventilated patients. Additionally, intubation is not a skill that nurses are permitted to perform or gain competency in and so less familiarity with the procedure may impact confidence in managing related equipment such as endotracheal tubes and ventilators.[21]
Infrequent exposure may have also impacted nurses’ low confidence in ECG interpretation despite nearly 90% confidence with cardiac assessments, as there is no dedicated paediatric cardiac unit and continuous ECG monitoring is not available on most of the paediatric units. Children with cardiac problems receive the same monitoring that other children receive: oxygen saturation, pulse rate, and temperature. Blood pressure and respirations are not routinely monitored in wards with high patient volume. Conversely, in the PICU at MJC, continuous monitoring is available, and the nurse-to-patient ratio is generally 1:1 or 1:2. Despite low confidence in ECG monitoring, most nurses (~ 80%) rated confident or somewhat confident their knowledge and use of vasoactive medications like adrenaline (used in cardiopulmonary resuscitation). When considering that many paediatric patients are very sick by the time they reach the hospital, the nurse’s confidence in using such a medication could be reflected simply by its frequency of use.
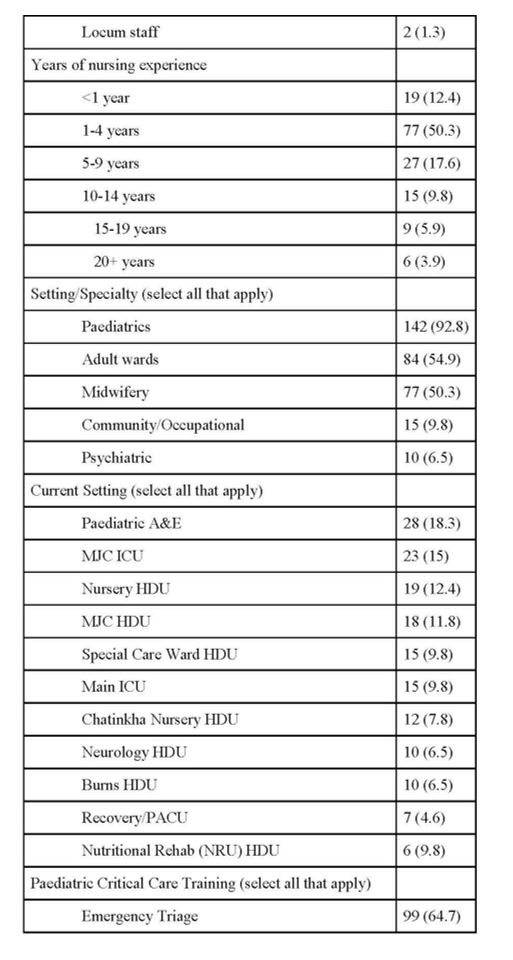
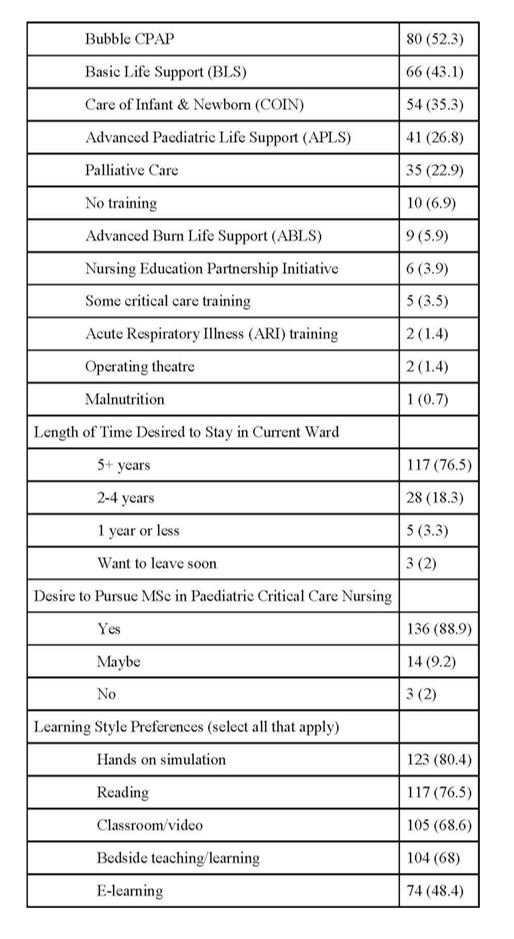
Considering effective learning styles for nurses, simulation has been shown to greatly impact nursing students’ self-efficacy and performance of nursing skills.[29] When asked about learning preferences, 80% preferred hands-on simulation and nearly half of nurses were interested in e-learning technologies, while 68% reported bedside teaching and classroom learning were preferred. Furthermore, combining learning styles has been shown to improve nursing students’ motivation, satisfaction, and subject-specific knowledge when compared to online-only learning.[30] Providing varied and accessible learning modalities through simulation, flipped classroom, and online curriculum will be important for ensuring success among nursing students as the PCC pathway is being created.
Research suggests that nurse retention in Malawi is negatively impacted by poor compensation, poor working conditions, high patient ratios, unsupportive managerial relationships, lack of career advancement, and lack of performance evaluation.[31] It has conversely been shown that nurse retention in rural settings is positively impacted by a clear career pathway, mentorship, and financial incentives.[32] In Malawi specifically there are strong religious and patriotic factors that increase retention.[31] Supportive work environments increase nurses’ job satisfaction, but have the added benefit of positively affecting patient and family satisfaction.[33, 34] Encouragingly, 76.5% of nurses had a desire to stay in their current ward for five years or more, and 89% of nurses were interested in pursuing a PCC master's degree (if funding were attainable). These findings may represent protective factors positively impacting nurse retention rates and a desire for specialization. Creating a PCC master’s pathway will give nurses an opportunity to acquire specialized skills which would encourage the MoH and hospital leadership to allow nurses to work within their area of expertise, improving nurses’ job satisfaction and ultimately patient care.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}