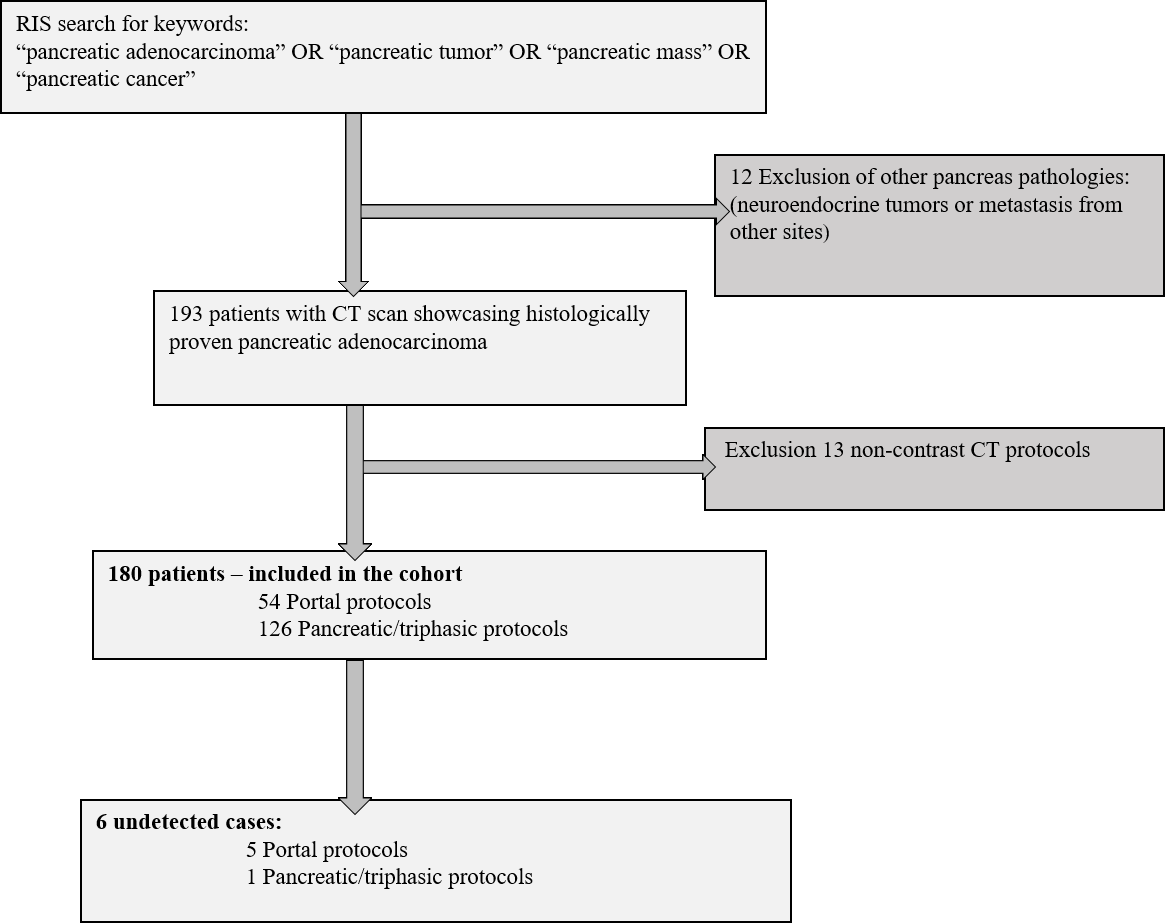
In this study, we have evaluated the failure to diagnose PDAC in different CT protocols. Our cohort included 180 patients, and found a miss rate of 9.3% of PDAC in portal CT scans. To the authors' knowledge, this is the largest cohort to investigate missed PDAC in abdominal CT scans, with reference to different CT protocols.
Kielar et al. described 13 errors that involved the pancreas out of 222 imaging errors, one of which was due to a missed pancreatic mass [16], and Donald et al. presented 558 diagnostic imaging errors, of which CT scans accounted for 43%, including 4 patients with missed pancreatic tumors [17]. These studies, however, did not analyze the rate of missed pancreatic tumors solely, and did not separate results according to CT protocols.
This study demonstrated significantly higher miss rate (9.3%) of PDAC in portal CT scans. Our findings are supported by current literature stating that pancreatic phase is superior in demonstrating pancreatic adenocarcinoma, due to better tumor-to-pancreas contrast [10-15]. In addition, the lower rate of missed pancreatic tumors on pancreatic and triphasic scans may also be attributable to radiologists being more conscious of subtle imaging findings when interpreting pancreatic/triphasic CT scans, which usually hold a stronger relation to the clinical question of tumor detection [18]. Since pancreatic adenocarcinoma is a lethal malignancy and early detection is the main chance of survival, physicians' knowledge of CT techniques is of crucial importance.
Several previous studies investigated the imaging findings of insidious pancreatic tumors [20-25]. Yoon et al. showed in their study of small (≤20 mm) PDAC, that approximately one-fourth of the small pancreatic masses were iso-attenuating. In that study, most of the small iso-attenuating tumors showed secondary signs; of which the most frequent were pancreatic duct abnormalities, including cut-off or dilatation [20]. Ahn et al. demonstrated that focal hypo-attenuation and pancreatic duct dilation with or without interruption were the most useful findings for avoiding delayed diagnosis of pancreatic cancer [21].
In our study, undetected tumors registered the following radiological signs: i) small (≤20 mm) hypodense lesions only retrospectively identified, ii) peri-pancreatic fat stranding and iii) dilated pancreatic duct with cut-off sign. We further recommend that these signs be emphasized in physician's training.
Errors in cancer diagnosis are likely the most harmful and expensive types of diagnostic errors [18-19]. Physicians should take into account the appropriate CT technique when there is clinical suspicion of pancreatic malignancy.
Our study has several limitations. This is a retrospective study, but only a retrospective study can present an accurate estimation of the miss rate of PDAC. Secondly, CT scans included in our work were done in several institutes, which reflect real life variability. Thirdly, the number of missed cases is small, though statistical significance has been observed.
In conclusion, the frequency of missed PDAC is higher on portal CT protocols. Physicians should consider the cancer miss rate on different CT protocols.
{kind=link}