Study Design
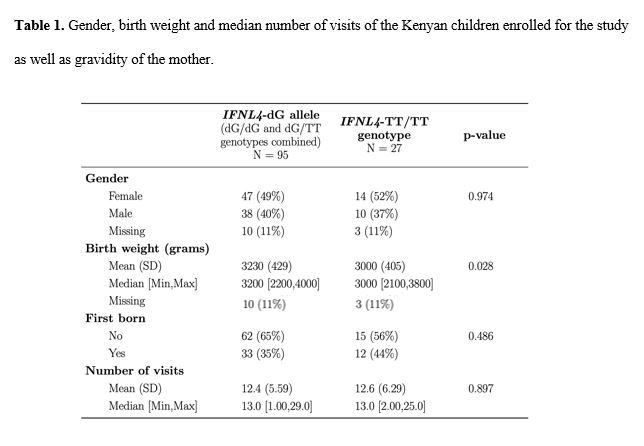
We used samples and clinical data collected by the Chulaimbo Antenatal Postnatal (CHAP) study, a prospective cohort study conducted in Kisumu, Kenya between 2011 and 2015. Details of this cohort have been described elsewhere [12,13]. Briefly, the study enrolled pregnant women aged 18-45 years presenting for antenatal consultation at Chulaimbo County Hospital (CCH). The eligibility criteria included HIV negative, singleton pregnancy and residency within ten kilometers of the hospital. If the participating women gave birth at CCH, newborn children were enrolled at delivery and underwent a newborn exam that included laboratory testing, a physical exam and anthropometric measurements. Children were followed for up to two years. The protocol and study procedures were approved by the institutional review board of the SUNY Upstate Medical University (where the study was initiated), COMIRB at University of Colorado, and the Scientific and ethical review unit (SERU) at KEMRI.
A health questionnaire was completed each time the child came for a clinic visit; children then underwent a physical evaluation and any medical findings were included in these questionnaires. URTIs were diagnosed by physical exam by the study clinical officer. X-rays and other diagnostic tests such as respiratory antigen testing for respiratory syncytial virus, influenza, parainfluenza or adenovirus were not available. It is also relevant to mention that lower respiratory tract infections and pneumonia were excluded. Clinical malaria episodes were diagnosed by clinical presentation and confirmed by blood smears to detect parasites in the blood.
Genotyping
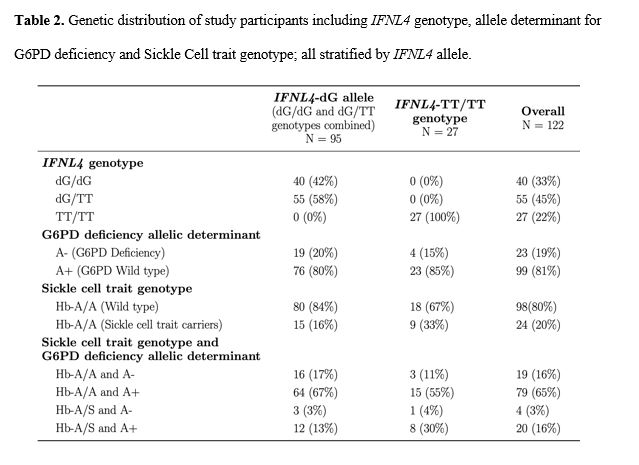
Genomic DNA was extracted from blood using DNeasy Blood & Tissue Kit (Qiagen) and genotyped for IFNL4-rs368234815 by custom TaqMan genotyping assays, using Genotype Master Mix (Qiagen), on BioRad iQ5, with standard conditions as previously described [4] (Image S1). Testing was performed blinded to clinical phenotypes.
Glucose-6-Phosphate dehydrogenase deficiency (G6PDd) was characterized as previously published [14]. Briefly, two PCR products, 352bp and 295bp, within the G6PD gene were amplified by PCR using the following primers: A- Forward (5’-CAGCCACTTCTAACCACACACCT-3’), A- Reverse (5’-CCGAAGCTGGCCATGCTGGG-3’), A+ Forward (5’-CTGTCTGTGTGTCTGTCTGTCC-3’) and A+ Reverse (5’-GGCCAGCCTGGCAGGCGGGAAGG-3’). The PCR amplicons were subsequently subjected to restriction enzyme digestion using NlaIII with resulting fragment sizes visualized by horizontal gel electrophoresis. For A- an uncut product was found from the normal locus, whereas two DNA fragments, 218- and 134-bp, were generated in the mutant locus. For A+ 2 DNA fragments, 243- and 52-bp, were found to be associated with the normal locus and 3 DNA fragments, 141-, 102-, 52-bp, were generated for the mutant locus.
Hb-A/S trait was characterized as previously published [15]. Briefly, a 772-bp PCR product within the human beta-globin gene was amplified from DNA extracted from whole blood using the following primers: HbB1 (5’-TCCTAAGCCAGTGCCAGAAG-3’) and HbB2 (5’-GAATTCGTCTGTTTCCCATTCTAAAC-3’). The PCR amplicon was subsequently subjected to restriction enzyme digestion using Bsu361 with resulting fragment sizes visualized by horizontal gel electrophoresis. A 430-bp DNA fragment was found to be associated with the mutant locus, whereas 228- and 202-bp DNA fragments were generated from the normal locus.
Statistical Analysis
Using data from questionnaires collected on all clinic visits, the relationship between malaria episodes and upper respiratory tract infections (URTI) with respect to IFNL4 alleles was evaluated. Only malaria episodes or URTIs that were reported on clinic visits forms were counted for. A Negative binomial regression model with an offset for the total number of sick and follow-up visits was used to evaluate the relationship between IFNL4 alleles and the number of infections; malaria episodes and URTIs were modeled separately. Estimates from the negative binomial model were exponentiated and reported as rate ratios. To evaluate the time to first malaria infection, a Cox proportional hazards model was fit using the survival package (v 3.1-8) [16,17] and survival plots were created using the survminer package (v 0.4.6) [18] in R. The final Cox model included adjustments for G6PDd and sickle cell trait with right-censoring at the end of the two-year study; the proportional hazards assumption was checked and was not violated. Adjustments for gravidity and maternal malaria exposure did not improve model fit or change conclusions about IFNL4 associations, so they were not included in the final cox proportional hazards model. To evaluate time to first URTI, Kaplan Meier estimators were calculated, and a log rank test was used to test for differences between IFNL4 alleles. All analyses were completed using R (version 3.6.0) [19].
{kind=link}
{kind=link}