This prospective observational study of patients with acute ischaemic stroke who were eligible for thrombolysis in a resource limited setting in Sri Lanka showed that nearly 10% died and that nearly 20% developed intracranial haemorrhages within 3 months of thrombolysis. Both on admission NIHSS and mRS were associated with functional dependence at 3 month follow up. Low dose rTPA administration was associated with a better NIHSS and mRS score at 3 months but it did not influence complications such as death or ICH, or shorten the hospital stay.
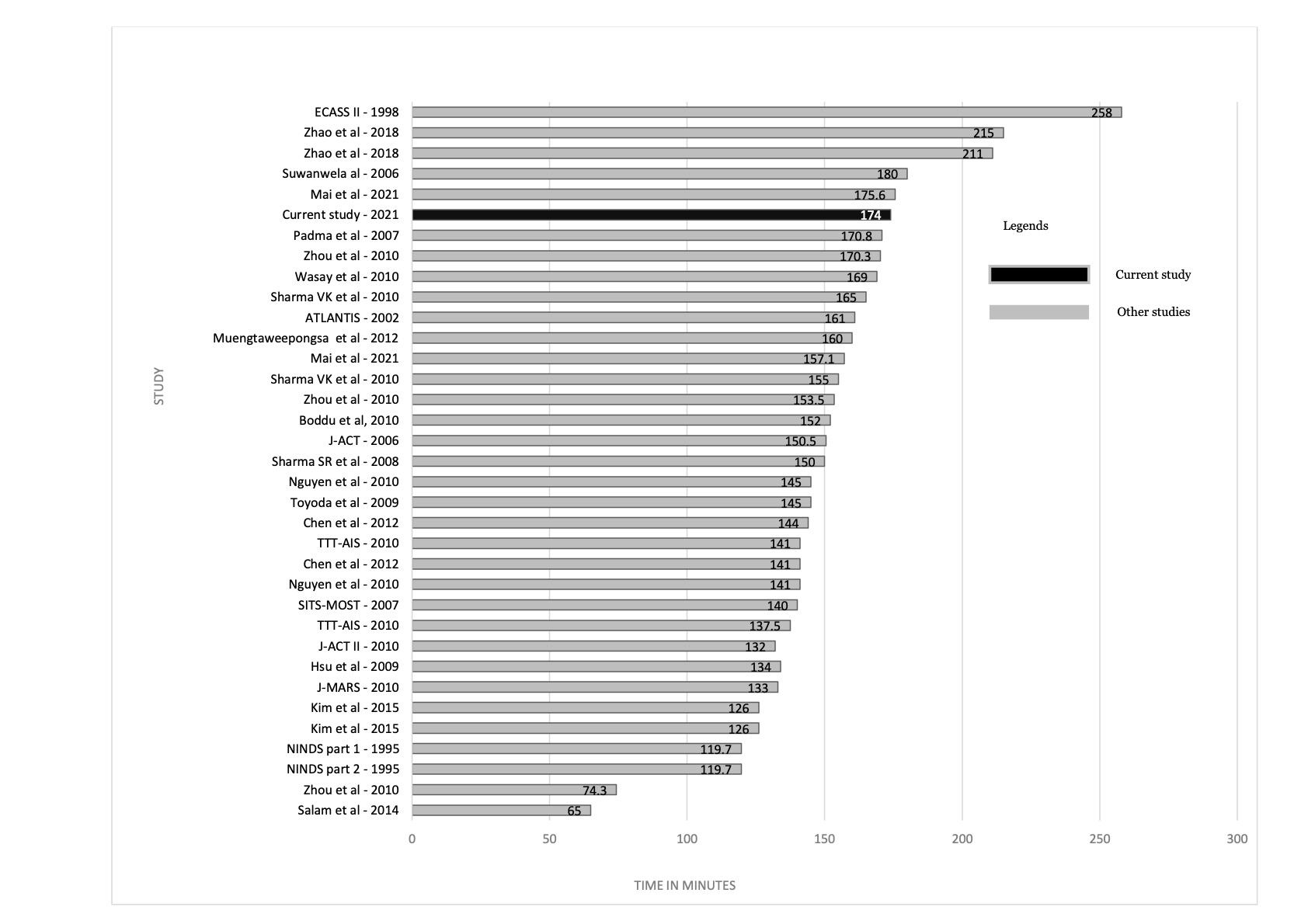
The age distribution and NIHSS on admission in the patient cohort of this study were comparable to those observed in other prospective studies on thrombolysis for stroke as detailed in supplementary table 2. However, the time from symptom onset to thrombolysis was comparatively higher (Supplementary Fig. 1). This may be due to delays in getting to hospital due to not using paramedic services, traffic congestion, living further away from the hospital or a combination of this factors. This study did not explore the reasons for delay in hospital admission, and also did not capture the people who came after the 4.5-hour time window to compare with, but this highlights the need for more qualitative and quantitative data to explore the reasons for delays in getting to hospital. Earlier thrombolytic treatment reduces in-hospital mortality and symptomatic intracranial haemorrhages while increasing functional independence following treatment 23, and it’s important that patients in resource limited settings can tap in to these benefits by timely access to healthcare.
A favourable outcome in terms of functional independence at 3 months post-thrombolysis in our patient cohort was associated with the on-admission mRS and NIHSS while the 3-month NIHSS was also associated with the presence of leukoaraiosis on the pre-thrombolysis CT scan. These observations agree with that of several previous studies 24–29. However, other studies have also found different associations for functional dependence/independence at 3 months such as major neurological improvement at 24 hours 24, pre-thrombolysis random blood glucose level 24, 25, blood pressure on admission29, cardiac ejection fraction 29, time to thrombolysis 25, patient age 24, 26, ASPECT Score on admission 26, hyperdense MCA sign30, 31, having an anterior circulation stroke 29 and past history of stroke / CHADS score 29. Some of these associations may be attributable to the variation in samples size and differences in baseline demographic and clinical characteristics (e.g., past history of co-morbidities) of individual cohorts. However, the time to admission (and thrombolysis) was associated with several outcome indicators in the unadjusted analysis in our cohort also. This association was insignificant in the adjusted analysis probably because as discussed above, due to the overall delay in getting admitted or treated compared to other studies. This should not be erroneously interpreted as time to admission (or thrombolysis) not having an impact on post-thrombolysis functional outcome. The overall variation in predictors across studies from different countries suggest that aiming to develop a universal system to predict post-thrombolysis functional improvements may be less relevant and instead clinicians should focus on establishing locally adapted, evidence based approaches to improve outcomes of their patients.
As for complications, the percentage suffering from post-thrombolysis sICHs were relatively higher in our cohort (supplementary Fig. 3) but the mortality was similar that observed in much larger international cohorts18, 32 (supplementary Fig. 4). This may be because we defined sICHs according to three different definitions (ECASS 2, SITS-MOST and NINDS trial definitions) and meeting any one of these definitions were considered as a positive case. Of these, SITS-MOST definition which only considers large parenchymal haemorrhage type 2 as sICH has had a good association with for poor outcome and mortality in previous studies 33, but we could not do a head-to-head comparison of these definitions due to low number of events observed. Previous studies have found several associations for post-thrombolysis sICH including age, current or historical antiplatelet /anticoagulant use 29, 34, 35, serum triglyceride and fibrinogen level 29, 36, statin use 37, 38, hypertension or hyperglycaemia on admission 29, NIHSS on admission 29, anterior circulation stroke 29, leukoaraiosis on CT 28, ASPECT score and comorbidities such as atrial fibrillation 29, renal impairment 39, heart failure 29 or a CHADS2 score > 2 29. Some of these associations have been confirmed in a meta-analysis 40. Interestingly, in this study we found a strong and independent association of lower BMI and sICH. This has not been observed before and currently we are unable to explain this observation, except that this observation should be confirmed in a larger cohort. Even though we found that hyperdense middle cerebral artery sign is significantly associated sICH ( relative risk of 3.74 ) several studies and meta-analysis have concluded that the association is not statistically significant30, 41, 42.
Whether low dose alteplase is comparable to standard dose in efficacy and safety in Asian patients remains controversial 43. The use of low doses of rtPA was proposed in Asian countries due racial differences related to the functionality of fibrinogen and coagulation factors which potentially increased the risk of intracerebral haemorrhage 43. Our observation was that low dose alteplase may be associated with better functional outcomes, but did not necessarily had a better safety profile with regard to deaths and sICH, as expected. Supplementary table 3 illustrates studies comparing low dose vs standard dose which mostly shows no difference for efficacy and safety outcomes. A previous meta-analysis had concluded that there is no association between alteplase dose and favourable outcome and mortality, but that the low dose may be associated with a lower incidence of sICH44. From a cost perspective, alteplase used in Sri Lanka is made in India and a 20 mg vial costs USD 355 while a 50 mg vial costs USD 692. If the low dose is as effective as the standard dose this could be considerably cost saving in a resource limited setting.
This study has several limitations; firstly, we recruited from a single centre which affects the generalisability of studies to the whole of Sri Lanka. Yet NHSL-c is one of the few centres where thrombolysis is available in the country and all other centres where thrombolysis is available also do have similar facilities and are supervised consultant neurologists. Secondly, Sri Lankan data may not be generalisable to other countries but as shown above in the discussion, the heterogeneity of associations for outcomes and complications highlight the need for locally relevant datasets than extrapolating findings from other countries. Thirdly, the sample size is small despite recruiting all eligible patients from all neurology units in the largest hospital in Sri Lanka located in the most populous district of the country over a 24-month period. This highlights a greater problem in gaining access to services within the critical time window for thrombolysis which may be influenced by patient-dependent (e.g., unawareness) and -independent factors (e.g., lack of infrastructure for faster transport of critically ill patients). Exploring reasons for this was beyond the scope of this study. Finally, comparison of low dose vs. standard dose alteplase should ideally be done as a randomised blinded controlled trial for conclusive results.
{kind=link}
{kind=link}
{kind=link}
{kind=link}