Study group
Ethical review board approval was provided by the institutional review board of University of Munich / LMU Munich, Protocol-Nr. 093 − 09. All examinations were performed in concordance with the Helsinki Declaration revised 2013.
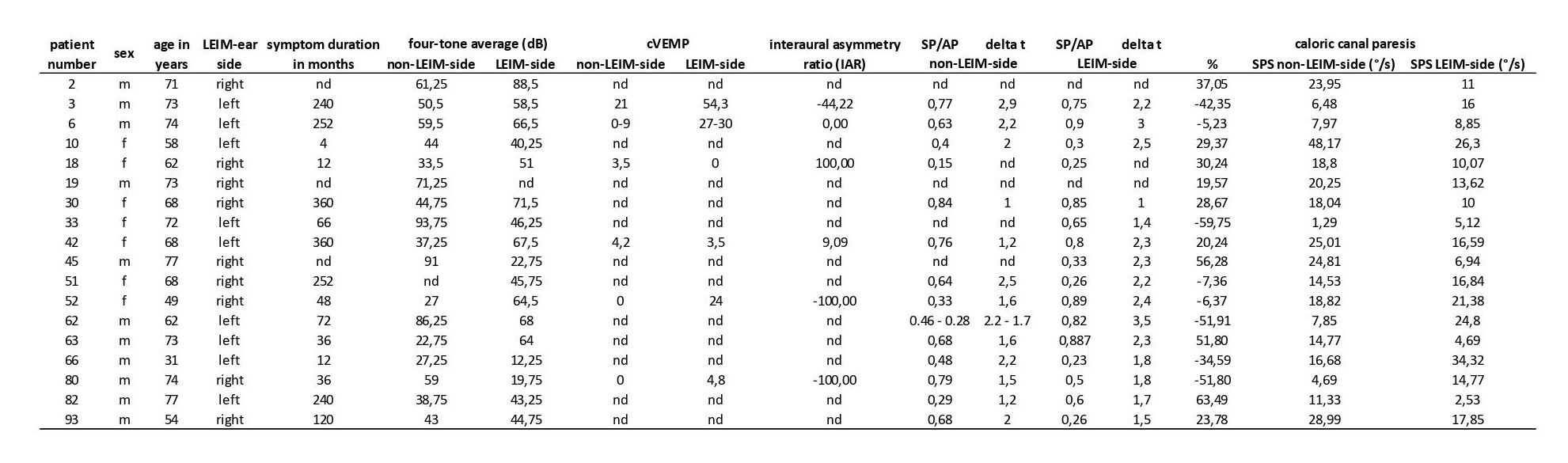
Patients with certain MD according to the AAO-HNS classification (1995)(23) and with MR morphologic confirmation of endolymphatic hydrops (ELH) as an equivalent to the required histopathological findings were included in the study (12, 24–26). All of these patients underwent MRI on a clinical 3 Tesla scanner investigation with a sequence protocol comprising several different MR sequences described below. All patients gave their informed consent for all the methods including them in the study, also for the locally enhanced inner ear MRI (LEIM) and the electrophysiological examinations. Morphometric analysis of the VIIth and VIIIth cranial nerves was performed retrospectively. 24 hours prior to the MRI scan a gadolinium-based contrast agent diluted 8-fold in saline solution, was intratympanically injected (27, 28). After administration, the patient remained in a supine position for another 30 minutes with the head turned approximately 45 degrees toward the contralateral side.
Patient data consisting of CISS-0.6-sequence measurements was compared in our previous study to clinical healthy controls (17). In the current study we compared the affected side with the non-affected side of unilaterally affected MD patients as well as the bilaterally affected MD patients vs. unilateral affected MD patients using the mentioned different MRI sequences.
MR Imaging
All MR imaging examinations were performed on a 3T MR unit (Magnetom Verio, Siemens Healthcare, Erlangen, Germany) using a commercially available 4-channel flexible surface coil combined with an 8-channel head coil.
The following MR-sequences were acquired of the temporal bone:
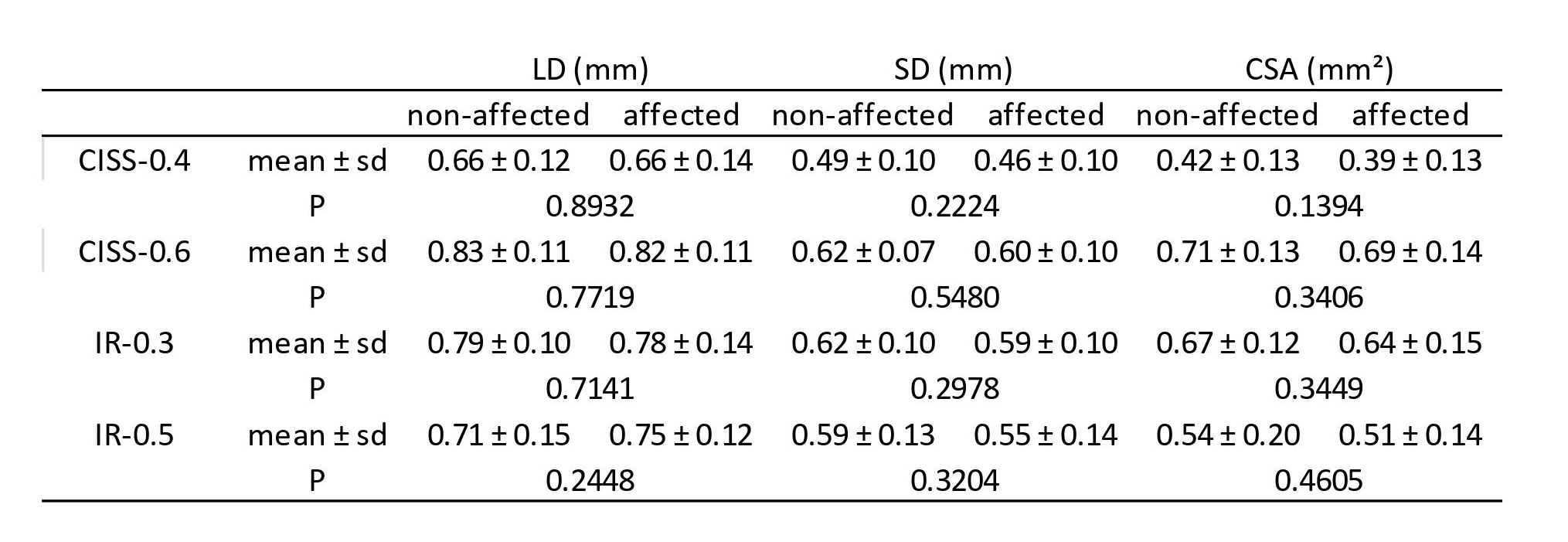
CISS-0.6: A strongly T2-weighted constructive interference in steady state sequence (CISS) with the following parameters was used: TR 7.2 ms, TE 3.16 ms, flip angle of 70°, field of view of 192 x 192 mm², matrix size of 320 x 320, averages 1 and slice thickness of 0.6 mm.
CISS-0.4: The second CISS had the following parameters: TR 6.24 ms, TE 2.87 ms, flip angle of 70°, field of view of 160 x 160 mm², matrix size of 320 x 320, averages 1 and slice thickness of 0.4 mm.
IR-0.5: The inversion recovery sequence was acquired using the following parameters: TR 6000 ms, TE 155 ms, flip angle of 180°, field of view of 160 x 160 mm², matrix size of 320 x 320, averages 1 and slice thickness of 0.5 mm.
IR-0.3: The second inversion recovery sequence had the following parameters: TR 6000 ms, TE 155 ms, flip angle of 180°, field of view of 160 x 160 mm², matrix size of 256 x 256, averages 1 and slice thickness of 0.3 mm.
Analysis
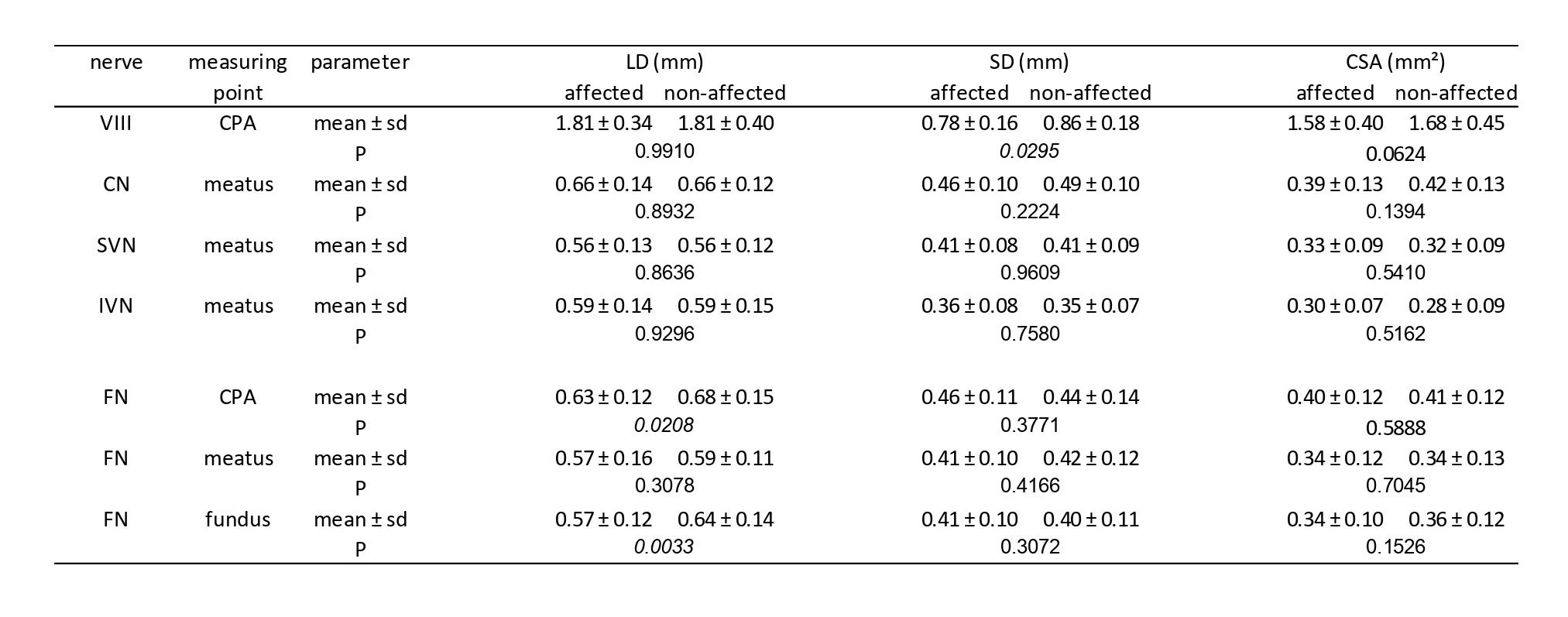
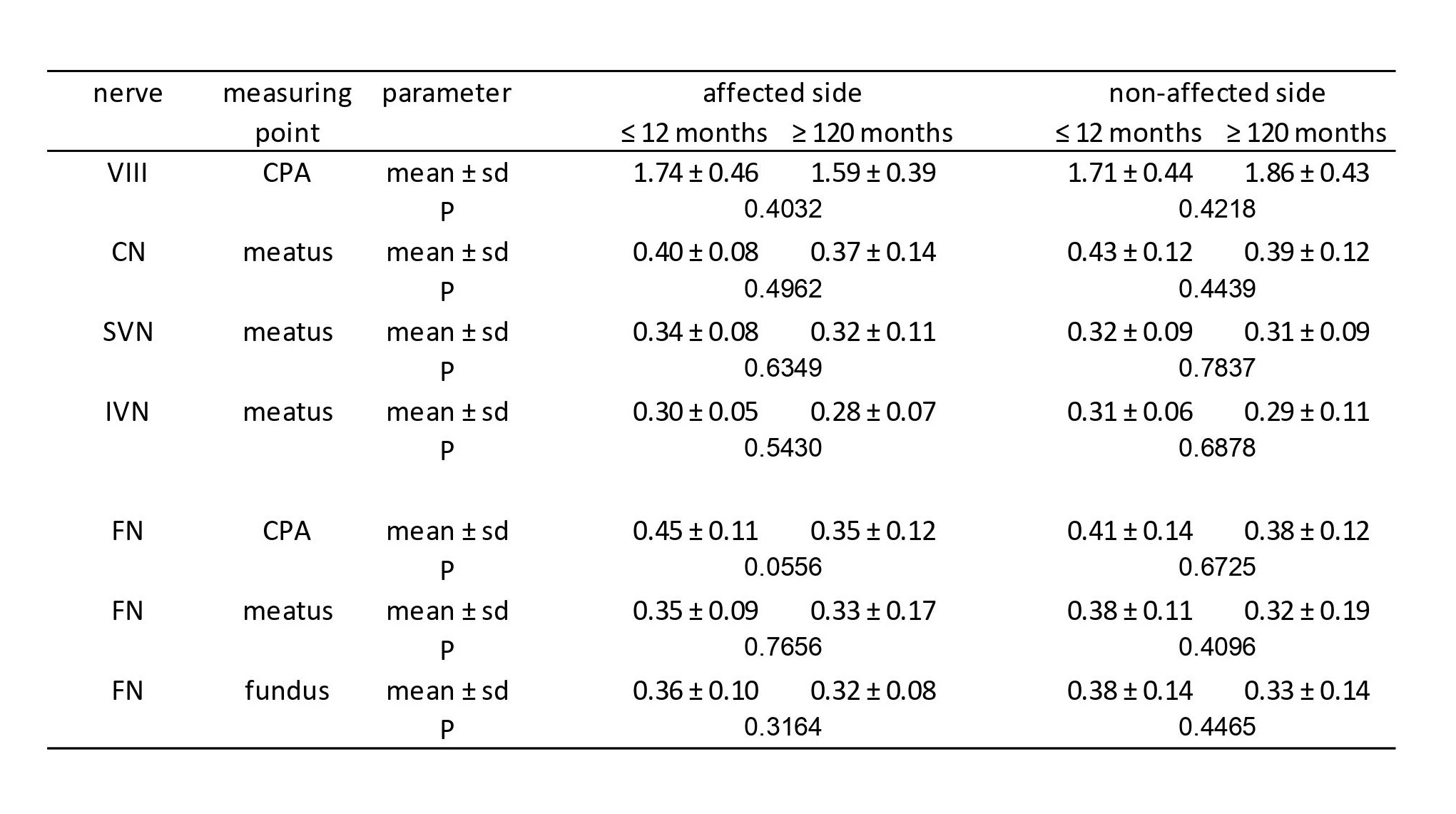
We used a commercially available DICOM-Viewer (OsiriX v.4.0, 64-bit version, Pixmeo, Switzerland) for measuring the diameters of the VIIth and VIIIth cranial nerves. Consistent windowing levels and thin slice thickness were used performing transverse reformats at different locations throughout the course of the nerves from the cerebellopontine angle (CPA) to the internal auditory canal (IAC) fundus. Locations of the transverse sections were defined as follows:
- VIII – CPA,
- CN, SVN and IVN - meatus of the IAC;
- VII – CPA, meatus of the IAC, fundus of the IAC.
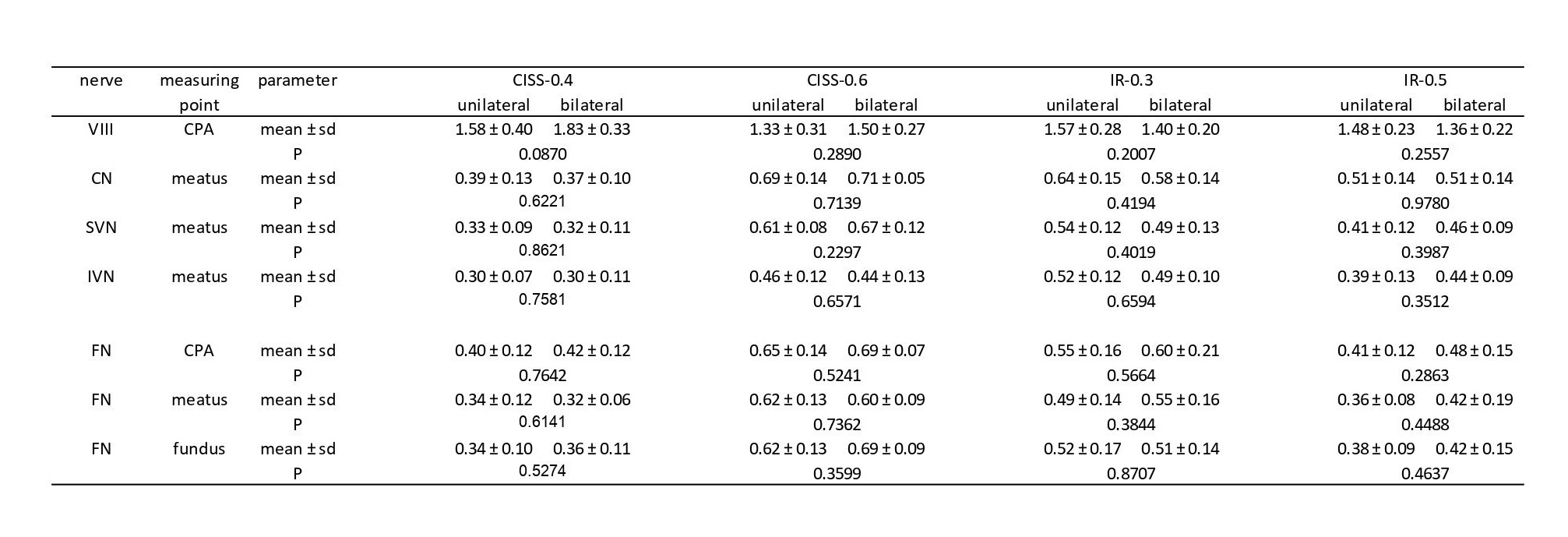
On each transverse section the long diameter (LD), short diameter (SD) perpendicular to LD and cross-sectional area (CSA) were measured. Several dot-markers were positioned on the outline of the examined nerves. These markers were linked and the CSA was calculated. All measurements were performed by the same two readers based on consensus readings. Both readers were blinded for the diagnosis of the patients. All these measurements were made for the CISS-0.4, the CISS-0.6, the IR-0.3 and the IR-0.5 sequences to investigate different nerve sizes depending on the used MRI sequence.
All patients received locally enhanced inner ear MRI (LEIM). The study group was subdivided into two cohorts: The first cohort consisted of unilaterally affected MD patients; the second consisted of bilaterally affected MD patients.
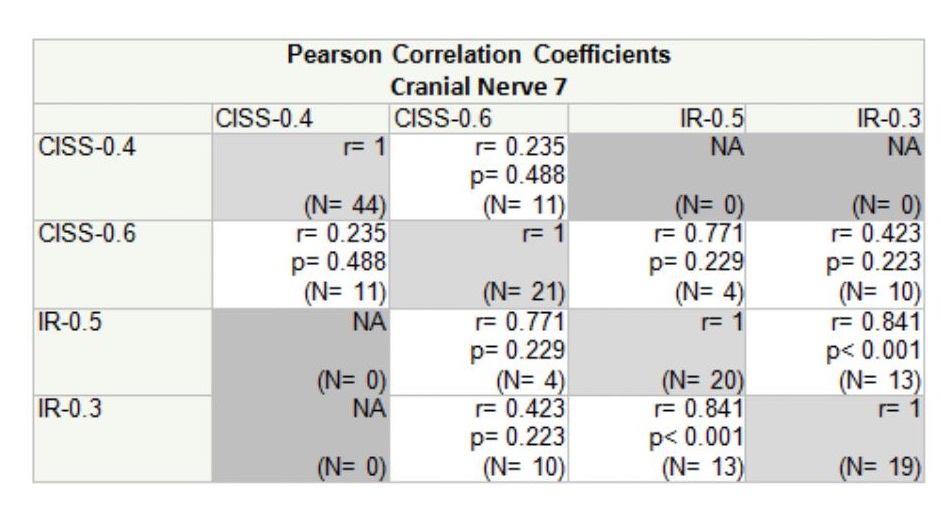
For comparing the affected and the clinically non-affected side a paired samples (dependent) t-test was employed using MedCalc v.12.7.2 (MedCalc Software bvba, Belgium) and SAS v. 9.4 for Windows (Copyright SAS Institute Inc., Cary, NC, USA). After Bonferroni correction P < 0.05 was reduced to P < 0.000595 for statistical significance. For comparing the subgroups of different symptom duration a two-sided independent samples t-test was used. Furthermore we used Scatterplots, Pearson Correlation Coefficients and Bland-Altman plots for visualization of the degree of correlation as well as measurement differences between the employed MRI sequences.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}