4.1 Main Results: The impact of Insulin Saturation:
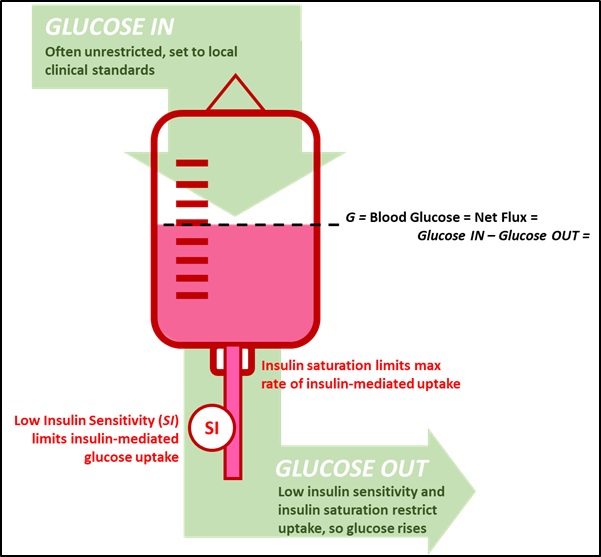
The analysis in Figures 4-6 clearly shows the trade-off between nutrition delivery, insulin saturation, and control to a specified blood glucose level. If insulin action was unlimited, where more insulin resulted in more insulin-mediated glucose uptake, nutrition could be independently set and a specified blood glucose level achieved as part of any standard titration problem. However, insulin action and effect is saturated [42,43,58-76], and increasing insulin doses eventually have less to no effect, except to raise plasma and interstitial circulating insulin levels. Hence, insulin saturation limits insulin-mediated glucose uptake, in turn limiting the total possible carbohydrate delivery to maintain a specified blood glucose level (Figure 5), unless blood glucose is allowed to rise (Figure 6). Thus, there is a patient specific, variable upper limit of carbohydrate delivery, which is a function of the patient’s insulin sensitivity (SI).
A high SI value indicates larger potential insulin-mediated glucose uptake is possible, and a low value a more resistant patient. Thus, highly insulin resistant patients, typical of ICU patients requiring glycemic control [1-3,5], are more likely to need lower nutrition delivery to maintain desirable glucose levels [91]. This outcome matches results showing lower mortality at reduced average nutrition delivery rates compared to current guideline rates [92-94], even though only a subset of more insulin resistant patients and/or patient hours might require such reductions from a typical goal nutrition delivery level.
Currently, nutrition delivery is most frequently set to local clinical standards for virtually all glycemic control protocols. Clinical insulin protocols are thus “carbohydrate blind”, neither knowing nor accounting for nutritional intake [95,96]. To date, only the model-based STAR and eMPC protocols consider nutrition explicitly [97-100], and only STAR modulates nutrition delivery in addition to insulin [98-100]. STAR and eMPC also directly identify patient-specific SI using virtual patient models [101,102], and can thus manage the entire trade-off in Figures 4-6 directly.
Clinical Impact: There are two clinical outcomes of Figures 5-6. The first is the clinical need to include nutrition delivery in glycemic management, whether or not it is controlled. The second is the clinical need to limit and optimise nutrition delivery for more insulin resistant (low SI) patients as a direct part of safely and effectively managing glycemia, where this restriction is increasingly seen as necessary in general [103,104]. As a result, model-based or similar methods to monitor insulin sensitivity (SI) directly could become more necessary to identify who, when, and how much nutrition should be reduced.
4.2 Main Results: The Impact of Metabolic Variability:
SI can vary significantly between and within critically ill patients [8,37,89]. Figures 6-8 describe the impact of SI variability on glycemic outcome and safety, and demonstrate the potential need to manage nutrition delivery to mitigate hypo- and hyper- glycemic risk.
Figure 7 illustrates the risk of SI variability, where critically ill patients have significant variability in their hour-hour insulin sensitivity, particularly early in ICU stay [89,105]. Hypoglycemic risk from rising SI ( ) can result in moderate or severe hypoglycemia in up to 10% of hours in the first 1-3 days of stay, depending on insulin dose [106]. The width of the potential variation is a function of insulin dose and nutrition rate given, where blood glucose level, insulin dose, and nutrition rate together magnify uncertainty in SI. The implication is smaller insulin doses, which can require lower nutrition rates, result in lower glycemic variability (Figure 8). Hence, more insulin resistant patients (lower SI) (Figures 4-5), with high blood glucose and insulin (and/or nutrition) rates may benefit from short-term reduction of nutrition to reduce both glycemic level and variability, as shown Figure 8.
Clinical Impact: Inter- and intra- patient metabolic variability in insulin sensitivity can significantly change the glucose levels resulting from any given insulin dose. The more insulin resistant the patient, the larger the insulin dose required, and thus the wider the resulting glycemic variability range resulting from changes in insulin sensitivity. Reducing nutrition, within clinically accepted ranges, is a means of managing this glycemic variability, and will be necessary for more resistant patients to mitigate avoidable hyper- and hypo- glycemic events resulting from metabolic variability.
Clinically, it is possible to quantify and thus account for this variability, creating an objective means to reduce hypoglycemic and hyperglycemic risk [89,105,107-110].
4.3 Limitations: Does Limiting Nutrition Reduce Total Nutrition Delivery?
Figures 4-6 illustrate the potential need to reduce or control nutrition delivery in managing glycemia patients with higher insulin resistance (lower SI). Nutrition delivery for the critically ill is an area with significant debate concerning the level of nutrition required, how much is practicable to deliver, delivery route, and the impact of macronutrients [92-94,104,111-121]. Recent analyses lean towards a staged approach, increasing nutrition delivery over ICU stay as patient condition improves, thus limiting nutrition delivery per protocol to lower than full or goal feed levels early in stay (e.g. [103,118,120]) when the greatest insulin resistance and variability most typically occur [8,37].
Figures 5-6 illustrate how insulin saturation limits insulin-mediated glucose uptake and thus limits the level of carbohydrate intake a patient can tolerate to avoid excessive hyperglycemia. The more insulin resistant the patient, the lower this value. Hence, at any given hour of stay, any given patient may be able to tolerate more or less carbohydrate nutrition intake than another otherwise similar patient, where a model-based SI value can differentiate such patients.
Currently, only the STAR protocol explicitly modulates insulin and nutrition to manage glycemic level and variability and risk due to Intra- and inter- patient metabolic variability [38,47,122]. Thus, the results in [91], showing mean nutrition during glycemic control met or exceeded leadin nutrition delivery over days 1-3 of ICU stay in a survey of 158 ICUs in 20 countries by Cahill et al [112], were surprising. Equally, a per-patient analysis showed a significant spread of maximum tolerated nutrition intake over the 221 patients (21,769 hours) in [91], where these patient-specific levels rose each day of ICU stay and faster than proposed in [103,118,120]. These results show how directly accounting for insulin sensitivity and insulin saturation, and its variability, can temporarily reduce nutrition delivery, but maximise overall nutrition delivery based on patient-specific tolerance, resulting in clinically very high levels of nutrition delivery despite controlling it to manage glycemia. More generally, limiting nutrition to improve glycemic control and minimise risk of glycemic variability does not have to limit total nutrition.
4.4 Clinical Takeaways:
The overall results show a relatively complex, often ignored, and difficult to measure trade-off. Highly insulin resistant patients are common and create the conditions where reducing nutrition is necessary. More succinctly, high and variable insulin resistance (low and variable SI) requires direct modulation and control of nutrition, in addition to insulin, to minimise the risk of excessive hyperglycemia and hypoglycemia. It can also result in high levels of overall nutrition delivery over the first 3-5 days of ICU stay, despite temporary reductions. This outcome and approach require model-based or similar methods to monitor insulin sensitivity (SI) directly at the bedside to understand for whom, when, and how much nutrition should be reduced. Overall, controlling nutrition inputs to provide safe, effective and patient-specific glycemic control is as much about optimising nutrition as it is about glycemic control.
{kind=link}