Different acute phase reactants (APRs) such as CRP, Serum Amyloid A (SAA) and ESR are used to monitor FMF patients [8]. CRP is readily accessible and affordable compared with SAA which is expensive and not widely available. Testing of SAA does not provide any additional information over CRP. Therefore, CRP seems to be adequate for follow-up of FMF patients [12]. CRP was the only APR increased in all attacks. Frequency of ESR was (88%), fibrinogen (63%), and WBC (50%) [13].
The aim of this study was to evaluate the association between acute phase reactants (hs-CRP) and ESR) and the genotype of familial Mediterranean fever gene (MEFV) mutations in FMF patients at the time of diagnosis and before starting treatment with colchicine. This may indicate if the hs-CRP and ESR can be used as cheap prognostic tools in evaluating FMF patients. To the best of our knowledge, this is the first report that discusses the importance of CRP in FMF patients upon diagnosis and before treatment.
Interestingly, this study showed a very strong association between hs-CRP and ESR and familial Mediterranean fever (FMF) compared with the healthy controls. This indicates the importance of evaluating hs-CRP and ESR in FMF patients when they are diagnosed and before starting the colchicine treatment and in the attack-free periods, which may give us an idea about the severity of the disease. A previous study showed that the white-blood cell count, CRP and IL-8 levels were higher in patients with FMF than in healthy subjects. Levels of ESR, fibrinogen, IgD, TNF-alpha, procalcitonin, IL-6, and C5a were not significantly different between patients and healthy subjects [14]. However, continuous elevation of acute phase reactants in FMF patients should be evaluated to prevent the development of amyloidosis [15].
In the current study, 12 known mutations in the MEFV gene were screened among 101 FMF Syrian patients which led to positive identification of 1, 2 or 3 mutations in 65 (64%) patients. The five most common mutations include M694V, V726A, M694I, E148Q, M680I (G/C) (Table 2). The five most common mutations detected in FMF patients with elevated hs-CRP include M694V, V726A, M694I, E148Q, M680I (G/C) (Table 2). The five most common MEFV mutations detected in this study are similar to what previously reported in the Syrian patients [5, 6, 16, 17] and the other Arab FMF patients [18] with different frequencies.
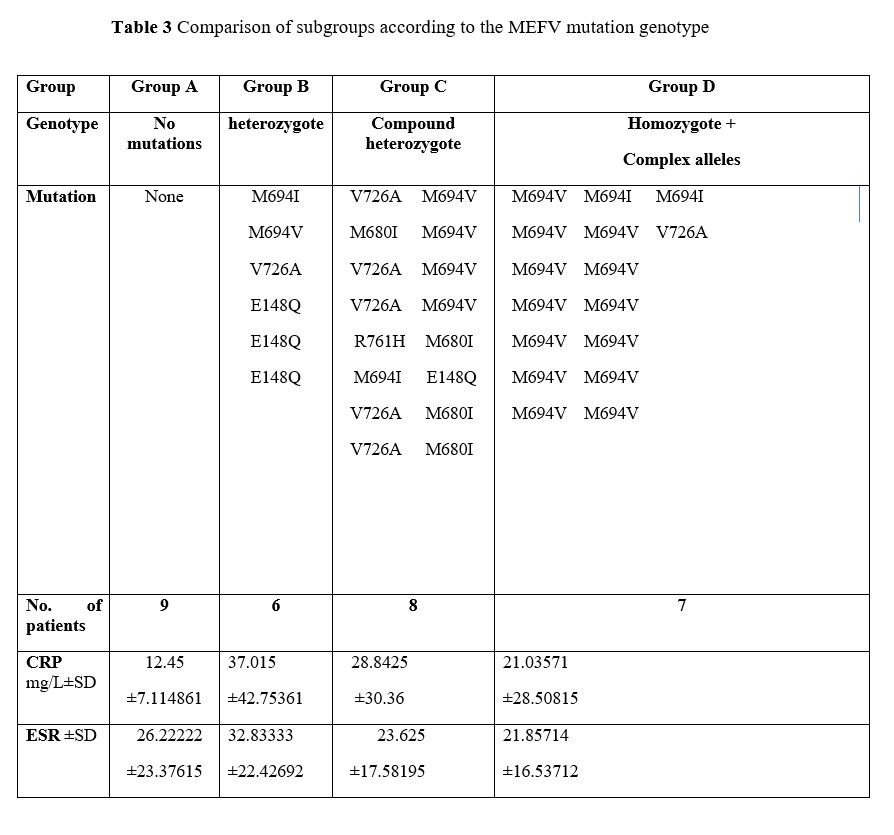
We Compared the MEFV genotype (group A (no mutations), group B (heterozygotes), group C (compound hetetrozygotes) and group D (homozygotes + complex alleles)) with the hs-CRP and ESR levels (Table 3). To the best of our knowledge, this is the first study that compares the MEFV genotype with the hs-CRP and ESR levels. We did not find any association between the MEFV genotype and the levels of hs-CRP and ESR. It has been previously shown that SAA and hs-CRP values were significantly increased in the patients with two mutations in exon 10 compared with the patients with one mutation in exon 10 which suggests an effect of gene dosage. Moreover, basal and peak concentrations of SAA and hs-CRP were highly increased in MEFV heterozygotes than in wild-type controls, regardless of mutation [7]. Kosan and colleagues have investigated the relationship between acute-phase reactants (ESR, CRP, fibrinogen, and white blood cell count) and gene mutations in attack-free periods of FMF children aged 2–18 years [11]. FMF patients’ samples were collected every 6 months for two years. Mean values for erythrocyte sedimentation rate and fibrinogen were statistically significant difference in the homozygous group. White blood cell count and CRP were similar in both groups.
We compared the M694V genotypes (group N (no mutations), group H (Compound heterozygote (M694V/Other) + Heterozygote (M694V/-)) and group Ho (homozygote (M694V/M694V) with the hs-CRP and ESR levels (Table 4). There were no statistically significant differences between these groups when comparing the ESR and hs-CRP levels. A previous study reported the association between the different MEFV genotypes and clinical features and cytokine inflammatory activity during the attack-free period in FMF patients and compared with the healthy controls [14]. There were statistically significant differences in FMF patients than in healthy controls with regard to the levels of CRP and White-blood cell count (WBC). Moreover, there were no statistically significance difference between the patients with M694V homozygous and heterozygous genotypes in terms of the WBC, ESR, CRP, fibrinogen and procalcitonin. Another study showed that FMF children with M694V homozygote genotype were associated with a higher acute phase response during FMF attacks and severe clinical symptoms [19]. It should be noted that both studies reported the acute phase reactant levels either during the attack free period or the attack-periods and not at the time of diagnosis like what we did in this paper.
Limitations of this study are the small size of the groups and short-term follow-up. Although we used hs-CRP and ESR as they are widely available and not very expensive, other APRs should be used in any future research in order to compare the results with each other.
{kind=link}