Study design and setting
The J-PICS study was a prospective, multicenter, observational cohort study of mechanically ventilated patients, conducted in 16 ICUs across 14 hospitals of Japan. Five of the 16 ICUs were university-affiliated hospitals, and the others were tertiary teaching hospitals. The median number of ICU beds was 10 [interquartile range (IQR), 8–15]. All ICUs were mixed ICUs and were managed by the intensivists. The study protocol was approved by the Kobe City Medical Center General Hospital (KCGH) ethics committee and the ethics committees of all participating hospitals (KCGH approval number: Zn181008). Written informed consent was obtained from all patients or authorized surrogates. The J-PICS study has been registered at University Hospital Medical Information Network Clinical Trials Registry (registration number: UMIN000034072).
Study population and eligibility criteria
All consecutive adult ICU patients who were expected to receive mechanical ventilation for more than 48 hours between April 01, 2019 and September 30, 2019 were recruited in the study. The patients who received noninvasive mechanical ventilation were also enrolled. Eligibility criteria were assessed next morning at 8:00 am after admission in the ICUs. The patients with the following conditions were excluded from the study: 1) patients who had primary brain injury that was likely to result in conscious or cognitive disorder (e.g., traumatic brain injury, subarachnoid hemorrhage, acute stroke, post cardiac arrest, meningitis, and encephalitis); 2) patients with pre-admission diagnosis of dementia; 3) patients who received home ventilation prior to admission; 4) patients with end-stage cancer; 5) patients with withdraw/withhold status; 6) expected death within 24 h; 7) second or subsequent admission to ICU during the study period; 8) patients who had no family members; 9) patients who did not speak Japanese; and 10) patients who could not be followed-up (e.g., did not live in Japan and/or were homeless).
Variables and measurements
The following demographic and hospital data of the patients were collected: age, sex, body mass index, Charlson comorbidity index (CCI) [18], clinical frailty scale [19], do not attempt resuscitation code status at the time of ICU admission, educational level, employment status, marital status, patient’s residential living status before admission, history of treatment with benzodiazepines and steroids, source of admission to ICU, and primary diagnosis at the time of ICU admission. We chose 9 years as the cut-off value for educational level because elementary and junior high school are mandatory for everyone, which usually last for 9 years in Japan, following which, many people go to high school for three years, followed by universities and graduate schools. The number of patients with sepsis and acute respiratory distress syndrome (ARDS) was also recorded. Sepsis and ARDS were diagnosed on the basis of Sepsis-3 [20] and Berlin definition [21], respectively. The severity of illness was measured using the Acute Physiology and Chronic Health Evaluation (APACHE II) score and Sequential Organ Failure Assessment (SOFA) score [22] within 24 hours of ICU admission. The management data in the ICU, including the use of inotropes or vasopressors, paralytic agents except during intubation, renal replacement therapy, extracorporeal membrane oxygenation (ECMO), intra-aortic balloon pump, and tracheostomy were also collected. The data for the use of inotropes, vasopressors, and paralytic agents were collected during the first four days of ICU admission. The data on patient outcomes, including ICU mortality; in-hospital mortality; length of stay in ICU; length of stay in hospital; duration of mechanical ventilation; occurrence of delirium, diagnosed by the Confusion Assessment Method for the Intensive Care Unit [23], during the first four days; and discharge status among survivors were collected.
Patient-reported outcomes
Six months after ICU admission, the authors sent the questionnaires by post to all patients except those who died. Patient-reported data were collected centrally. If the participants did not revert, the lead author asked each participating institution to attempt a contact via telephone to return the questionnaire.
The patient-reported outcome survey evaluated the physical and mental functions of patients through the assessment of HRQOL and cognitive functions. HRQOL was assessed using the SF-36 questionnaire [24–26], which is available in the Japanese language [27,28]. At the time of enrolment in the study after ICU admission, the patients’ baseline SF-36 questionnaire was completed by a proxy (4-week recall assessment before the patients’ current acute illness). At 6 months after ICU admission, SF-36 questionnaire was obtained by mail from the patient or proxy. The SF-36 questionnaire has established acceptability, reliability, and validity in critically ill patient populations and as a surrogate-completed proxy measure [29–36]. SF-36 questionnaire is a comprehensive 36-item survey of HRQOL with two summary scales, physical component scale (PCS) and mental component scale (MCS), with scores ranging from 0 to 100. A higher score indicates better physical and mental functions. Both scales were transformed to a normalized scale using norm-based scoring (NBS) with 50 as the population mean and 10 points representing one standard deviation. The scores were calculated based on the standard methods [37]. The missing data were treated using the standard methods. If a patient answered more than half of the items on the subscale, the missing data were replaced with the mean of the subscale. In contrast, if a patient answered less than half items on the subscale, the data of the answered questions were excluded [37].
Cognitive functioning was assessed using the Short-Memory Questionnaire (SMQ) [38]. The SMQ was to be completed by a proxy, similar to the Informant Questionnaire on Cognitive Decline in the Elderly [39]. The SMQ is the only questionnaire filled by a proxy that has been translated and established in the Japanese language [40]. The SMQ is a 12-item questionnaire with scores ranging from 4 to 46. A score less than 40 indicates cognitive dysfunction.
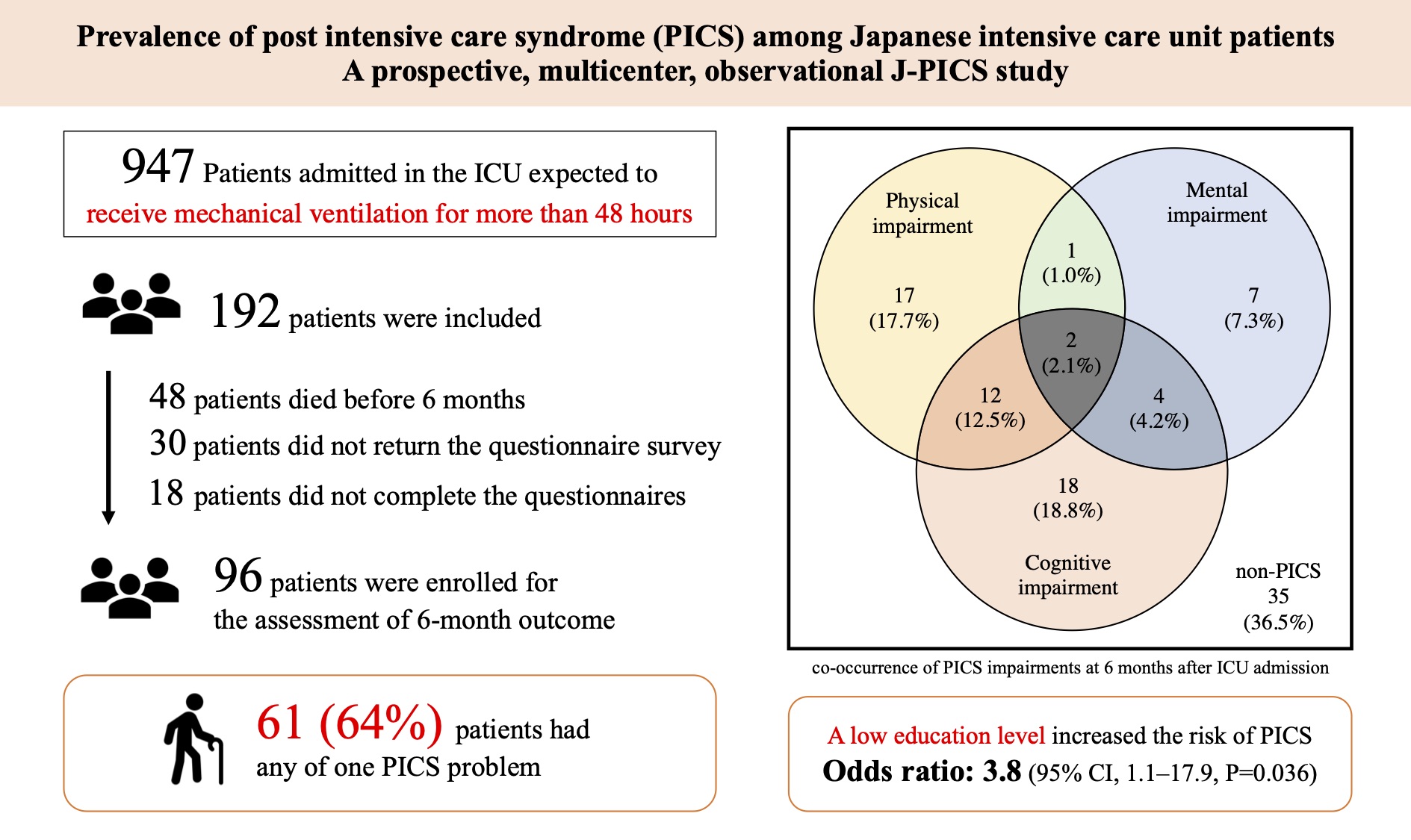
The primary outcome was the occurrence of PICS 6 months after ICU admission. The definition of PICS was any of the following criteria: 1) decline in physical status, indicated by PCS score decrease of ≥ 10 points; 2) decline in mental status, indicated by MCS score decrease of ≥ 10 points; or 3) cognitive function impairment, indicated by decline in SMQ score and SMQ score < 40 at 6 months after ICU admission. A 10-point change was considered clinically important in a previous study in the ICU setting [36]. For the assessment of subjective significance of SF-36 score change, participants also answered anchor questions on whether their physical and mental status had improved, worsened, or remained unchanged on a 7-point Likert scale (from large negative change to large positive change) [41–43] at 6 months. The questions related to patients’ employment status at 6 months were also asked.
Statistical analyses
Since the analyses focused on patient-reported outcomes at 6 months, participants who were lost to follow-up and who died before 6 months were excluded from the final analysis. Sample size was based on the total number of patients meeting the inclusion criteria because this prospective study was descriptive and hypothesis generating by nature. Continuous variables are presented as medians and interquartile range. Categorical variables are presented as absolute values and percentages. A univariate analysis was performed using the Wilcoxon rank-sum test for continuous variables, and the chi-squared test or Fisher’s exact test was used for categorical variables, if the number was less than 10. Multivariate logistic regression model was used to identify the factors associated with the occurrence of PICS. Multivariate analysis included the following variables as confounding factors: age, APACHE II score, CCI, and educational status [7, 44–46]. Age, APACHE II score, and CCI were log-transformed. The risk of PICS is expressed as odds ratio (OR) with 95% confidence interval (CI). The number of missing data have been reported, and no assumptions have been made except for SF-36 questionnaire data. The changes in SF-36 PCS, MCS, and SMQ scores between baseline and 6 months after ICU admission were compared using the Wilcoxon signed-rank test.
The subjective significance of change in SF-36 PCS and MCS was assessed by an anchor-based question with a Global Assessment Rating as large negative change, moderate negative change, small negative change, no change, small positive change, moderate positive change, and large positive change in physical and mental status. The change in each Global Assessment Rating for SF-36 PCS and MCS scores is expressed as mean and standard deviation (SD). Further, we evaluated the responsiveness of SF-36 PCS and MCS. Responsiveness is the instrument’s ability to detect change over time in the construct to be measured [47,48]. Responsiveness of SF-36 PCS and MCS scores to negative change or no change in Global Assessment Rating at 6 months was calculated using the effect size index [49,50]. Cohen’s d effect size was used to evaluate the changes as small (0.2–0.49), moderate (0.5–0.79), and large (> 0.80) [47,51]. We also assessed interpretability, which is the degree to which one can assign qualitative meaning to the quantitative scores or change in scores. We also evaluated the floor effect and ceiling effect of SF-36 PCS and MCS scores. Floor and ceiling effects were calculated as the percentage of participants scoring their lowest and highest (0 and 100) score, respectively. The floor and ceiling effects were considered relevant at 15% [52]. The minimal clinically important difference (MCID) of SF-36 PCS and MCS scores was calculated as the mean change score for no change patients minus the mean change score for small negative change patients [53,54].
The differences with P value less than 0.05 (two-sided) were considered statistically significant. All data were analyzed using JMP 15.1.0 (SAS Institute Inc., Cary, NC, USA).
{kind=link}