Medical ICU practitioners and hospital administrators may prepare for a potential surge in critical care capacity during the global COVID-19 pandemic by optimizing workflows for rapid diagnosis, isolation, clinical management as well as addressing concerns relating to supplies and infrastructure [17]. However, these preparations must also focus on the ICU staff, including protection from nosocomial transmission [18]. This is particularly crucial with hypoxic COVID-19 patients requiring non-invasive respiratory support, including NIV and HFNO, since these may generate aerosols composed of small virus-containing particles, depending on factors such as duration of use, oxygen flow velocity, mask leakage as well as patient coughing and cooperation [19]. Our study was conceptually innovative in attempting to explore bedside TDC insertion as a viable alternative in order to help prevent hospital-acquired infections without compromising patient safety or quality of care. We describe a series of 25 patients infected with COVID-19 requiring kidney replacement therapy that underwent bedside placement of right IJ TDCs in the ICU, using only ultrasound and anatomic landmarks without fluoroscopic guidance.
The standard of care for TDC insertion dictates that the procedure be performed under ultrasound and fluoroscopic guidance to ensure fewer catheter placement related complications and adequate catheter function [6]. Complications arising from TDC insertion including catheter related infections and thrombosis contribute significantly to patients’ morbidity and mortality at a considerable economic burden on society [8, 20]. The hypercoagulable state of patients with COVID-19 also makes them potentially more vulnerable to thrombotic complications and catheter occlusion [21, 22]. Furthermore, it is important to ensure that the patients are comfortable whilst they are placed in the supine position in order to improve cooperation during the procedure and reduce the risk of insertion failure or catheter mal-positioning [23]. However, it may be challenging to provide a balanced analgesic strategy during TDC placement to provide adequate discomfort relief whilst ensuring respiratory and cardiovascular stability, especially in patients on respiratory support requiring conscious sedation. Therefore, we implemented certain precautionary measures into our protocol for bedside TDC placement in patients with COVID-19 to mitigate the risk of developing catheter related complications.
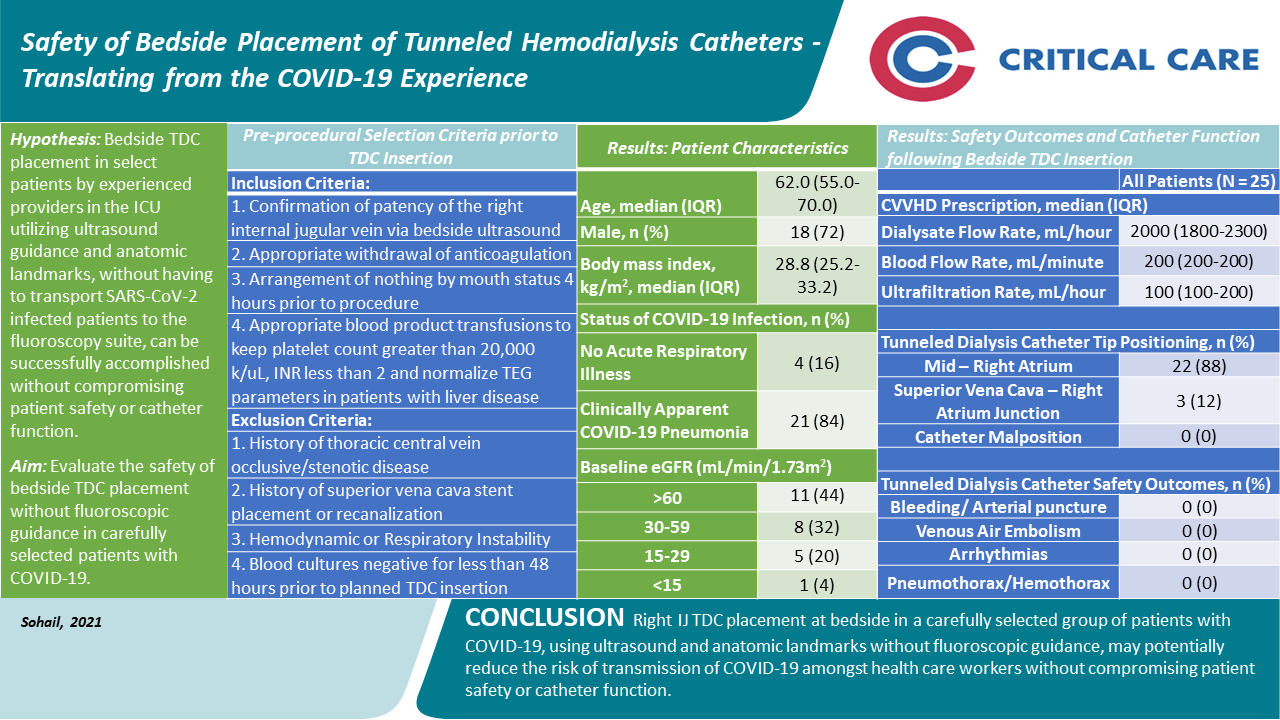
Firstly, we developed rigorous selection criteria for patients with COVID-19 under consideration for TDC insertion in an attempt to identify ideal candidates. In addition to excluding patients with absolute contraindications to TDC insertion including sepsis/bacteremia and uncontrolled coagulopathies [6], we also did not attempt bedside TDC placement in patients with new onset cardio-respiratory instability or with a history of central vein stenotic/occlusive disease.
Secondly, we selected the right IJ vein as the preferred site for bedside TDC placement to further try to minimize the risk of catheter dysfunction and placement related complications. Blood flow rates are consistently higher with right-sided jugular venous catheters than with left sided catheters since placement of catheters into the left IJ vein requires that the catheter make two right angled bends as well as an antero-posterior bend over the pulmonary arch prior to reaching the SVC [24]. There is additional resistance to flow not only from the multiple bends but also from the longer length of the catheter on the left-side. A retrospective analysis of jugular venous catheters depicted that left-sided IJ venous catheters had higher rates of infection (0.50 vs 0.27; P = .005) and catheter dysfunction (0.25 vs 0.11; P = .036) compared with those inserted from the right [25]. Therefore, the longer path that a left sided catheter has to traverse, predisposes it to developing catheter dysfunction as opposed to a right sided catheter, which has a relatively shorter, less meandering course to the SVC.
Utilizing our protocol and implementing the aforementioned safety measures, we were successfully able to place TDCs at the bedside in patients with COVID-19 requiring kidney replacement therapy and achieved adequate catheter blood flow rates without any deviation from the CVVHD prescription or evidence of catheter occlusion/dysfunction. Furthermore, no catheter placement related complications were observed and none of the catheter tips were mal-positioned on post-insertion chest radiographs. The acute escalation in the proportion of critically ill COVID-19 patients with acute kidney injury and the overwhelming need for urgent kidney replacement resources, coupled with the prospect of having to transport all these patients outside the ICU to the fluoroscopy suite for TDC placement mandated the consideration of bedside TDC insertion. In addition to protecting hospital personnel from COVID-19 exposure by limiting transportation needs, we further limited potential nosocomial transmission amongst health care workers by eliminating the involvement of multiple teams for the procedure.
Moreover, we were able to concomitantly place tunneled central venous catheters (small bore [5 Fr]; single or double lumen) along with TDCs in the right IJ vein in 10 of our patients, potentially further reducing personnel exposure to COVID-19. The prospect of concomitant placement of multiple catheters in a single central vein may ignite concerns regarding increased risk of catheter-related complications including infections and thrombosis as well as puncture related complications such as pneumothorax. Furthermore, with concomitant placement of a small-bore central venous catheter with a central hemodialysis catheter, there may even be concerns regarding hemodialysis catheter dysfunction. However, one retrospective analysis [26] compared patients who had undergone concomitant placement of a hemodialysis catheter and a central venous catheter for infusion with patients who only had a hemodialysis catheter placed in their right IJ vein. No significant differences were found between the aforementioned two groups of patients in the incidence of thrombosis (1.0 % vs 0.0%, p > 0.999), line infection (2.1% vs 0.0%, p = 0.519), or line dysfunction (2.1% vs 0.0%, p = 0.516). No puncture related complications such as pneumothorax were reported for either group. Therefore, even though multiple catheters are not routinely placed in the same central vein, the simultaneous placement of multiple catheters may be considered if necessary, without increasing the risk of complications.
It is encouraging to note that another case series at a tertiary community-based medical center has also reported successful placement of 24 bedside TDCs by the institution’s vascular surgery department [27]. Only one patient out of the series developed a catheter placement related complication, which was pneumothorax and cardiac tamponade. Some important distinctions between our studies include: (a) some of their TDC insertions utilized fluoroscopic guidance requiring movement of the patient to a fluoroscopy compatible bed whereas only ultrasound was used in all our procedures for real-time guidance (b) chest radiography was utilized at the time of sheath insertion in their series with a median of 5 plain radiographs taken during TDC insertion, whilst only one post-procedure chest radiograph was performed in our patients for confirmation of catheter tip position (c) we have clearly stated the selection criteria for patient candidacy for bedside TDC insertion to identify ideal candidates in an attempt to mitigate the risk of catheter related complications (d) concomitant placement of TDCs and tunneled central venous catheters in the right IJ vein was performed in our series.
{kind=link}