The recent outbreak of the COVID19 pandemic is caused by SARS-CoV2 virus which has affected substantial proportion of world population and has a high mortality, especially in the elderly. In the symptomatic patients, it can cause respiratory distress and hypoxemia that may require hospitalization (1). Total active cases of COVID19 in India stand at 411133, and the case fatality rate of reported cases is 2.7% (https://www.mohfw.gov.in/). However, case fatality rates of symptomatic COVID19 cases hospitalized needing immediate care in various hospitals across India is still unknown.
Multiple risk factors associated with SARS-CoV-2 and the development of COVID-19 could contribute to the increased severity and earlier onset of acute ischemic stroke including generalized hypercoagulability, dysregulated immune response leading to cytokine-release syndrome, damage to endothelial cells leading to increased inflammation and thrombosis, dysregulation of the renin-angiotensin-aldosterone system, direct cytotoxic effect on the nervous system related to angiotensin converting enzyme-2 (ACE-2) receptor uptake of SARS-CoV-2 virus, hypoxemia related to cardiorespiratory failure and metabolic derangements. The purpose of these case series is to provide an overview of SARS-CoV-2 and the mechanisms related to the development of thrombosis that led to the morbidity and mortality associated with COVID-19, including acute ischemic stroke. Reported rates of arterial thrombosis range from 2.8% to 3.8% (10).
While numerous mechanisms of thrombosis have been proposed, there is activation of the innate immune system in response to introduction of a viral pathogen. This immuno-thrombosis is the interaction between the innate immune system and thrombosis (11). It focuses on interplay between activation of intravascular TF, innate immune cells, platelets, endothelial cells and releases neutrophil extracellular traps (NETs) which can activate the contact pathway of coagulation. This concept is a cornerstone for the main hypothesis underlying COVID-19-associated coagulopathy.
MOLECULAR PATHOGENESIS OF THE POSITIVE SENSE VIRUSES
Coronaviruses are positive sense RNA viruses which have a remarkably high pathogenicity and infectivity. These viruses directly translate their mRNA into proteins after they encounter host ribosomes. These positive sense RNA viral genomes can directly translate their protein into the host cell and process of replication of the virus begins in the cell. This leads to interactions between host translation factors (proteins of the host cell or ACE2 in a patient) and RNA replication at multiple levels after entry of the virus (2). The process of replication is started by the genes for RNA-dependent RNA polymerase (RdRp) that is utilized by all these positive strand viruses after infecting the host cell. The genomic RNA is translated by messenger RNA (mRNA) to produce polymerase and positive-strand RNA viruses use additional replication factors for membrane targeting, template recruitment, RNA capping, and other functions (3-5).
Internally, virus gains entry through 2 routes:
- Direct entry: This happens when the virus directly lands on the 40S ribosome of the start AUG codon to make the protein. This helps the virus to form a new protein as soon as it encounters the host cell. After the protein is formed, the virus starts replication and with the help of other internal proteins and internal machinery the proteins get modified for further replication.
- Indirect entry: This happens when the virus gains entry next to the start AUG codon and the viral protein and host protein combine to form a new modified protein. These modified proteins are needed for replication (6,7).
Certain host ribosomal glycoproteins are loosely attached to the rough endoplasmic reticulum. These proteins create linear polymers of amino acids called polypeptides. These proteins are involved in the structural functions of the cell wall or membranes as receptors, for other molecules to bind. These are conjugated proteins having hydrophilic nature. Viruses also have glycoproteins that have an important function as it avoids the host immune system. Viral envelope with the help of glycoproteins identifies and binds to the receptors of the host proteins on the cell membrane. It fuses with the host membrane, allowing the capsid and genome of the virus to enter and infect the host. Glycation plays a key role in the viral replication and avoidance of the immune response. Glycosyl transfer can also occur to protein residues, to give O-linked glycoproteins and N-linked glycoproteins and enzymes like glycoside hydrolases or glycosidases break glycosidic bonds. Enveloped viruses enter their host cells by a process of membrane fusion. This fusion can occur at the cell plasma membrane or within the endocytic vacuolar transport, depending upon the characteristics of the virus fusion protein. Each of these virus-host interactions are host specific, tissue specific and dynamics of infections. Each such virus-host interaction also represents a potential target for virus control. Mutations in another host gene, OLE1 (OLEic acid requiring), also block RNA replication after membrane association of 1a, 2a polymerase, and viral RNA. OLE1 is an essential gene encoding Delta9 fatty acid desaturase, the key enzyme for converting saturated to unsaturated fatty acids. This enzyme is found in the endoplasmic reticulum of the host cell (8-10).
MECHANISM OF ENTRY THROUGH ANGIOGENESIS
Angiogenesis is the formation of microvasculature, a highly important mechanism of normal physiological events like pregnancy, menstruation, organ transplants and wound repair (1,2). This mechanism is being appreciated in inflammatory processes, apart from tumor nutrition in various cancers including benign processes. Oncogenes have been implicated in inducing the expression of angiogenic factors like vascular endothelial growth factor (VEGF) (3,4). Severe viral and bacterial infections have been known to induce increased angiogenesis in-vivo and these viral infections result in neoplasia and increased angiogenesis in part through viral-specific oncogenes. The viral infections most commonly studied with increased angiogenesis in-vivo are Papovaviruses (Simian virus 40, human papillomavirus) and Herpesviruses (Epstein-Barr virus) (5-9).
The importance of the two pathways essential for angiogenesis are VEGF and its receptor VGFR and ANG (Angiopoetin) with its receptor TIE (tyrosine kinase with immunoglobulin-like and EGF-like domains) which help in regulating both physiological and tumor angiogenesis. Hence, experimental drug inhibitors of both ANGPT2 and VEGF in some tumor models have been more effective than inhibition of a single pathway. Furthermore, combination of inhibition of VEGF and ANGPT2 may help to overcome the challenges in current anti-angiogenic therapies and particularly in viral infections like COVID-19 (39). Angiopoietin 1 and 2 regulate angiogenesis and vascular remodeling by interacting with the tyrosine kinase receptor TIE 2, and inhibition of angiogenesis has shown to be landmark in inhibiting virus induced cytokine response . The ANG 1 and ANG2 inhibitors could be potential pathway in blocking angiogenesis along with the vascular endothelial growth factor.(VEGF). ANG1 and ANG2 are peptide monoclonal antibody that inhibit binding of angiopoietin 1 and 2 to TIE 2, thus inhibiting angiogenesis.
IMMUNOMODULATION OF COVID 19
Toll like receptors(TLR) pathways play a major role for activation of innate immune system, secreting proinflammatory cytokines like interleukins(1, 6, Tumour necrosis factor and Interferons). Blocking the TLR pathway could lead to decreased secretion , thus helpful in controlling COVID 19 infection.
The coagulation cascade has been found to be activated during viral infections. Studies have shown that the activation may be part of the host defense system to limit spread of the pathogen. However, excessive activation of the coagulation cascade can be deleterious. In fact, inhibition of the tissue factor/factor VIIa complex reduced mortality in a monkey model of Ebola hemorrhagic fever. Other studies have shown that incorporation of tissue factor into the envelope of herpes simplex virus increases infection of endothelial cells and mice. Furthermore, binding of factor X to adenovirus serotype 5 increases the infection of hepatocytes and activation of the innate immune response to the virus. Hence Coagulation x inhibitors would be helpful in reducing the innate immune response. In cellular studies it has been observed that coagulation proteases activate protease-activated receptors (PARs) and subtypes PAR1 and PAR2 modulate the immune response to viral infection. For instance, PAR1 positively regulates TLR3-dependent expression of the antiviral protein interferon β, whereas PAR2 negatively regulates expression. These studies indicate that the coagulation cascade plays multiple roles during viral infections.
INFLAMMATORY MARKERS IN SEVERE COVID 19 INFECTION
Lactate dehydrogenase (LDH) is an inflammatory marker which has been detected in nasopharyngeal secretions during viral upper respiratory infections (URI) and in the middle ear effusions of patients with otitis media (5,6,7,8); Some studies have demonstrated it to be a biomarker of severity of inflammatory cellular injury during viral URI. The nasopharyngeal cellular injury can arise from a multitude of factors during viral URI; these include direct virus-induced cytopathic injury of the infected cells and participation of leukocytes such as neutrophils, macrophages, and lymphocytes in both antibody-dependent and antibody-independent cytotoxicity (10). A variety of chemokines and cytokines, specifically the acute-phase cytokines such as IL-1β and TNF-α, and other soluble mediators can act on the local endothelial and epithelial tissues to enhance the migration of the leukocytes toward infected epithelial cells, which in turn, participate in the cytotoxic injury of infected cells as well as nearby bystander cells (40).
Some studies have shown Azithromycin to be highly effective in reducing muscle enzyme Creatine Kinase, Lactate Dehydrogenase, Interleukins (IL-4, IL-6, IL 10 ), levels of C reactive protein(CRP) and increase levels of CD3+, CD4+ and CD8+ after treatment.(Zhang Jing and Yang Hui)
Serum ferritin is a well-known acute-phase reactant, denoting acute and chronic inflammation in infectious, rheumatologic, hematologic and malignant disease. In general, serum ferritin is glycosylated and has a high ratio of Ferritin light chain (FTL) to Ferritin heavy chain (FTH) whereas intracellular ferritin is not glycosylated (43). The FTL has a site for N-glycosylation, which is die to post-translational modification of the protein as it moves through the Golgi apparatus to its site of secretion (44). Additionally, the relative contributions of glycosylated and non-glycosylated ferritin to serum levels are also altered during a disease. Normally, the glycosylated fraction (GF) of serum ferritin is ~50%. But the recorded elevations in serum ferritin are accompanied by low levels of glycosylation, typically ≤20% (45–48) in certain severe infections, hemophagocytic syndromes and drug-induced hypersensitivity reactions, regardless of etiology (49–51), (52, 53) (50). However, the degree of glycosylation may help distinguish underlying pathology (42).
Drugs that have been effective in treatment and severity of COVID 19 are:
DRUGS
Azithromycin (AZT) is a macrolide and a phospho-glycoprotein inhibitor which has a very important role of transportation of viruses, bacteria and drugs into the cells of the body, which the viruses need for replication. Higher doses have been studied for their role as antiviral and the capabitlity of this macrolide to stop the replication and reduce proinflammatory markers. (40) The lung epithelium, which produces interferons (IFNs) upon infection with virus like retrovirus, is the mainstay in the antiviral defense of the lung and leads to the stimulation of interferon genes that directly interfere with virus replication (13, 14). Cellular studies have shown that IFN-1 is important for host defense against certain retroviruses, and treatment with endogenous IFN showing reduction in viral load in-vitro cell culture cells (15–17). This highlights the importance of IFNs as therapies to control replication of retroviruses in the lung alveolar cells and highlights the potential of IFN inducers such as Azithromycin as treatment for virus-associated exacerbations, even in patients of cystic fibrosis.
Azithromycin pre-treatment reduced viral replication in cystic fibrosis bronchial cells, due to the antiviral response via the IFN pathway.
In conclusion, the antiviral effect is achieved only after increasing the dose demonstrated by the exposure of lung and bronchial washing to azithromycin by doubling the dose to 1000 mg, which results in more effectiveness of the drug in the lower respiratory tract (43).
Pentoxifylline (PTX) is a methylxanthine derivative having a highly significant role in management of deep venous thrombosis and intermittent claudication.. (11). It has been shown to have anti-inflammatory, antiviral, immunomodulatory and bronchodilator properties in many molecular studies (12-14). PTX has also been found to be have broad spectrum anti-viral activity, through prevention of viral replication and has been used as an anti viral agent against viruses like herpes simples, rotavirus, vaccinia virus, human immunodeficiency viruses (HIV), SARS, etc. (15-18).
D dimer is the by product of fibrinolysis and PTX increases cAMP levels in polymorphonuclear leukocytes, decreasing micro vascular thrombosis and haemorrhage and also has an important function of an anti-inflammatory agent by inhibiting the production of pro-inflammatory cytokines. (19-22). It also acts as bronchodilator by reducing blood viscosity and increasing red blood cell flexibility thereby making it easier for them to migrate through narrow capillaries rapidly, increasing blood circulation (23-26). This creates perfusion and enhances oxygenation to all the tissues and organs including lungs as it halso has a role of a bronchodilator. Being widely available and cost effectivity, it can be a promising drug target for SARS COVID-19 treatment, either alone or in combination (25, 27-29).
Pro-inflammatory cytokines released by stimulated macrophages in the alveoli could have a prominent role in pathogenesis of SARS. Previous studies on treatment of SARS with antiviral agents such as ribavirin and corticosteroids have not achieved very satisfactory results. Corticosteroids exert an anti-inflammatory effect and are indicated for the treatment of respiratory distress, but on the other hand, they exert an immunosuppressor effect on humoral and cellular immunity. PTX could have an antiviral role along with immunomodulating effect, down-regulating proinflammatory cytokines but not effecting the immune response.
Itraconazole (ICZ) is an anti-fungal agent has also been recently explored as a potential treatment option for COVID-19. It’s an anti-fungal, increases the expression of P glycoprotein (transporter protein), THE MAINSTAY IN THE VIRAL GLYCOPROTEIN PATHWAY.
This drug inhibits Lanosterol 14α-demethylase (CYP51A1) which is a cytochrome P450 enzyme
It has been found to be effective against a wide range of viruses like rhinoviruses etc. (30-32). Recent studies show its role against type 1 feline coronavirus infection .(33). ICZ acts by interfering with the ergosterol synthesis pathway of the host cell thereby inhibiting cytochrome P450 enzyme, the lanosterol 14α-demethylase, which impairs cholesterol homeostasis (34-36). This disruption in the sterol synthesis shifts IFN-1 expression levels, accelerating the virus-induced host cell response. IFNs often serve as the first line of defence against viral infections. ICZ inhibits proliferation of endothelial cells by inhibition of 14-demethylase and sterol biosynthesis (37).The sterols like cholesterol are the chief components of the lipid pathways and play a central role in the viral entry into the host cells. Through these lipids, viral genome fuses and releases into the host cell. Viruses attack the host lipid pathway and and upregulate them to enchance their own replication thus form a viral cell membrane (38, 39). Hence, targeting the lipid metabolism pathways in the way that ICZ does could constitute an early-intervention option for SARS-COV2 cases.
It’s a highly effective anti-angiogenesis factor where in it acts by inhibiting VEGF A and C through their receptor VEGFR and plays an important role in inhibiting other inflammatory cytokines (Figure 1). This could also be used with PTX as a preventive therapy for SARS COV2.
Ceftriaxone is a highly potent phospho-glycoprotein which also induces interleukin-10 action. The anti-inflammatory effect of IL-10 is critical to protect the host from tissue damage during acute phases of immune responses. Hence the viruses can evade immunity by hijacking this regulatory mechanism and cause tissue damage in the acute phase. This regulatory interleukin can be produced by almost all cells involved in the immune mechanism., and it has a very important action of immune modulation. The cytokine has very complex and multifunctional in inflammatory response to acute viral infections. There are various factors involved in IL-10 production and the cellular sources of the cytokine during antiviral immune responses. IL-10 regulatory mechanisms have an impact on antiviral immune responses and how viruses can use this central regulatory pathway to evade immunity and establish chronic infections, hence these regulatory mechanisms play an important role in fulminant viral infection, and are highly important factors to be considered in COVID 19 infection. Antiviral immune responses ideally eliminate replicating virus and viral reservoirs without host damage. However, in many infections, severe complications could occur due to excessive immune activation. To prevent host tissue damage, immunoregulatory cytokines control the magnitude of these immune responses. IL-10 is a key component of this inflammatory mechanism that regulates and suppresses the expression of proinflammatory cytokines during the recovery phases of infections and consequently reduces the damage caused by inflammatory cytokines
Dexamethasone is a long acting immune modulatory steroid which has been shown to be have lifesaving properties in COVID-19 patients. Dexamethasone therapy leads to a rapid, clinically beneficial effect that may be due to upregulation of IL10 production and strong immunosuppressive effect, which is most evidently observed in the decrease in Interferon gamma., and enhances T2 cell activity. In vitro evaluation showed that this shift in T cell balance was a direct effect of dexamethasone and thus independent of the hypothalamic-pituitary-adrenal axis. It has an inducing effect on the CYP3A4 activity and hence should not be given concomitantly with Itraconazole.
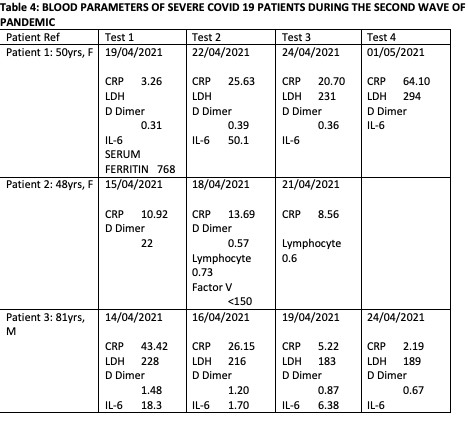
Comparative profile of severe patients in SECTION 1 and SECTION 2
In the first section we report a comparative profile of a total of five severe cases with varied co-morbidities managed through combination of above repurposed drugs over a period of 14 days. These drugs have been combined with other Phospho-glycoprotein inhibitors like Pantoprazole, Metformin for Diabetes, Telmisartan for hypertension, Amiodarone for arrythmias specific for the comorbidities. And Nitazoxanide for gastrointestinal system involvement.
In the second section we have discussed case histories of severe patients with and without comorbidities affected with the double mutant virus strain that has been causing a very high mortality We studied the effectivity of these combination drugs in the double mutant viral strain during the second wave affecting Indian community and causing severe symptoms in these patients
{kind=link}