Survey Results
Participants’ ratings resulted in six of the 36 QIs listed in the survey being more important: (1) increasing the quality of life of patients; (2) increasing healthcare staff skills; (3) decreasing patients’ symptoms; (4) decreasing family caregiver burden; (5) increasing patient satisfaction with care; and (6) increasing family doctor continuity of care (Table 3).
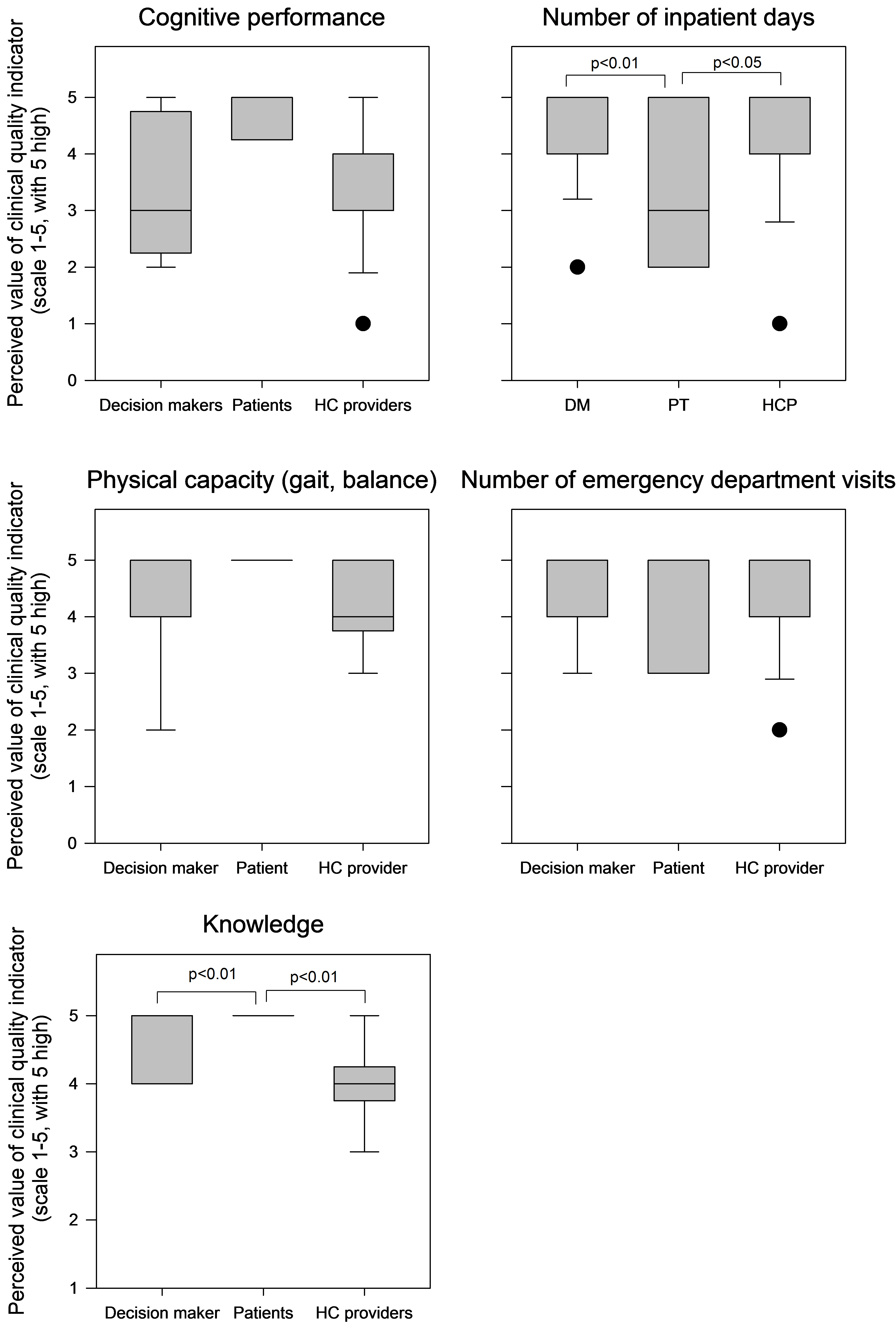
The ratings of five other QIs, notably the number of inpatient days during the last year of life, rate of emergency department visits, physical capacity (gait, balance), provider knowledge, and cognitive performance varied by type of participant. Specifically, a post hoc analysis showed that older adults placed less value on the number of inpatient days during the last year of life, but valued provider knowledge more compared to HCPs and DMs. Variations were not statistically significant for the rate of emergency department visits, physical capacity, and cognitive performance (see supplementary material).
Participants’ Motivation for the Ratings
In the interviews, participants explained their motivation for assigning their ratings of top-rated indicators. The majority emphasized the importance of improving patients’ quality of life, and considered this indicator as far more important than, for example, decreasing risk of death. Participants shared a strong feeling that older adults with frailty must be able to define their quality of life, because that allows them to define their own care goals and meet them accordingly. Overall, all participants viewed this indicator as essential to raise awareness about older adults’ perspectives in the process of care. Participants also suggested that quality of life should be measured and reported along with other patient-reported outcomes.
I think they all ultimately play into quality of life and what the patient and their loved ones, their caregivers, feel that’s important... what’s important to them. (Alberta, DM#3)
Healthcare providers’ skills were rated close behind quality of life. Participants shared concerns that poor or deficient skills may limit the quality of care and services older adults with frailty receive, as well as their quality of life. Participants also discussed what the term “skills” included, and suggested that awareness and support in providing assistance with activities of daily living should be considered an essential skill.
An increase in the provider’s competency or skills, that’s another side of the equation, but if you are looking strictly at the quality of a clinical intervention, certainly, increasing the knowledge and skills of the people delivering that clinical intervention should result in a strong increase in quality. (Alberta, DM#4)
Participants considered it important to decrease symptoms since they can influence patient autonomy and quality of life. They expressed concern that symptoms, especially pain, often remain undetected by HCPs and are underreported by patients. Therefore, participants suggested that symptoms must be assessed thoroughly as part of a geriatric assessment.
I think reduction of symptoms, certainly. That is going to be an indicator of better quality of life in most instances, again, if I think of palliative care patients. If the symptoms are better managed, there is usually a better quality of life […]. (British Columbia, HCP #4)
Participants also prioritized the need to decrease the burden on family caregivers. According to them, family caregivers are overworked and need support, however, the issue remains largely unaddressed at this time. Participants stated that a sustainable healthcare system relies on family caregivers to help keep older adults with frailty at home, manage their quality of life, and avoid institutionalization and, therefore, caregiver burden must be measured and reported.
If we don’t understand how to reduce caregiver burden, we’re not going to have a sustainable system. So that is really, really, really important, I think, from everyone’s perspective. (Alberta, DM #2)
Participants explained that older adults with frailty and HCPs might not have the same views about patient satisfaction regarding care, and that this indicator helps obtain patients’ views on several other important indicators, such as quality of life, caregiver burden, or patient coping effectiveness and autonomy. Consequently, some suggested that “experience with care” would be a more appropriate indicator than “patient satisfaction”. Although some expressed concerns with patient satisfaction being a subjective measure, the majority valued this indicator because it provides insight into older adults’ views and experiences with care.
For me, “patient satisfaction with care,” I would maybe reframe that to “satisfaction with their experience with the system of care,” because some older adults will say, if it’s the care which is actually the nurse at the bedside or the care in the home, yes they are satisfied … but surrounding that care is a system with which they’ve had great frustration. (British Columbia, DM #4)
Participants viewed continuity of care provided by a family doctor over the last year of life of the older adult with frailty as important because family doctors know their patients well, they are there for older adults, and are perceived by participants as partners in the care of older adults with frailty.
I think that the family physician piece [of the puzzle] is important, particularly for those who have long-standing relationships with their family doctors. […] They often know the individuals very well and I think the more we can tap into that, the more we can often make a difference in the quality of care. (British Columbia, HCP #4)
With the exception of continuity of care, participants perceived that practical measurement of the highest-rated indicators may not be feasible.
{kind=link}