Study patients. This prospective study included consecutive patients with chronic HF referred to our outpatient clinics in Pisa for clinical evaluation and follow-up from 2010 to 2019. The inclusion criteria comprised LV EF ≤ 50% and LV end-diastolic volume (EDV) index > 75 ml/m2.
Exclusion criteria were: recent myocardial infarction or unstable angina (< 3 months), coronary artery bypass graft or percutaneous coronary angioplasty (< 3 months), more than mild aortic or organic mitral valve disease, cardiac valve lesions requiring surgical and/or percutaneous repair, planned cardiac resynchronization therapy, hypertrophic cardiomyopathy, amyloidosis, active myocarditis, prosthetic valve dysfunction, and inadequate image quality. Patients with atrial fibrillation were not excluded from the study. The study was approved by the local institutional review board. All patients gave written informed consent with their approval to participate in the study. The study was conducted in accordance with the institutional policies, national legal requirements, and the revised Helsinki declaration.
Clinical evaluation. The patient's functional status was determined according to the classification of the New York Heart Association (NYHA). Blood was drawn for natriuretic peptides (NP), B-type natriuretic peptide (BNP) and amino-terminal proB-type natriuretic peptide (NT-proBNP) assays, and measure of renal function. Blood pressure, heart rate and rhythm were recorded. The estimated glomerular filtration rate was calculated from the simplified formula derived from the Modification of Diet in Renal Disease (MDRD) study.
Echocardiographic examination. Transthoracic two-dimensional and Doppler echocardiographic examination (including tissue Doppler) was carried out with an iE33 X5-matrix and an EPIQ 7 Ultrasound instrument (Philips, Andover, Massachusetts) equipped with a 3.5-MHz transducer. The following standard echocardiographic variables were obtained: LV volumes and EF and left atrial volume index (LAVi), were assessed from apical two- and four-chamber views using the biplane Simpson's method. From mitral velocity tracings, peak early (E) and late (A) transmitral flow velocities, their ratio E/A, and E wave deceleration time (EDT) were measured from spectral Doppler recordings of LV filling. Doppler tissue imaging longitudinal velocities were recorded with the sample volume placed at the junction between the septal and lateral LV wall and the mitral annulus in the 4-chamber view. A ratio of E/averaged myocardial early velocity of the lateral and septal sites (averaged E/e') was calculated. Tricuspid annulus plane systolic excursion (TAPSE) was measured from M-mode recordings. Retrograde blood flow of tricuspid regurgitation was recorded using continuous-wave Doppler for measuring peak tricuspid regurgitation velocity (TRV). The peak velocity was assigned as the average of five tricuspid regurgitation envelopes with the greatest maximal velocities and spectral density. The ASE-EACVI 2016 recommendations were used to estimate normal or increased LVFP[11] The LV outflow tract (LVOT) anteroposterior diameter was measured in the parasternal long-axis view, and the LVOT area was estimated as π(d/2)2 (cm2). LV stroke volume was calculated as the product of the LVOT area and the velocity-time integral of the forward flow. LVOT velocity-time integral was measured by tracing the outer edge of the densest (or brightest) portion of the spectral tracing with the pulsed wave Doppler sample volume positioned in the middle of the LVOT below the aortic cusps from the apical 5-chamber or long-axis view, and CO was calculated as stroke volume multiplied by heart rate[12]. Cardiac index (CI) was estimated by dividing CO by body surface area. For each Doppler-based measurement, estimates were obtained from 3 cardiac cycles in sinus rhythm or 5 in patients with atrial fibrillation. Mitral regurgitation severity was graded using the vena contracta method or by measuring the effective regurgitant orifice area into mild, moderate and severe.
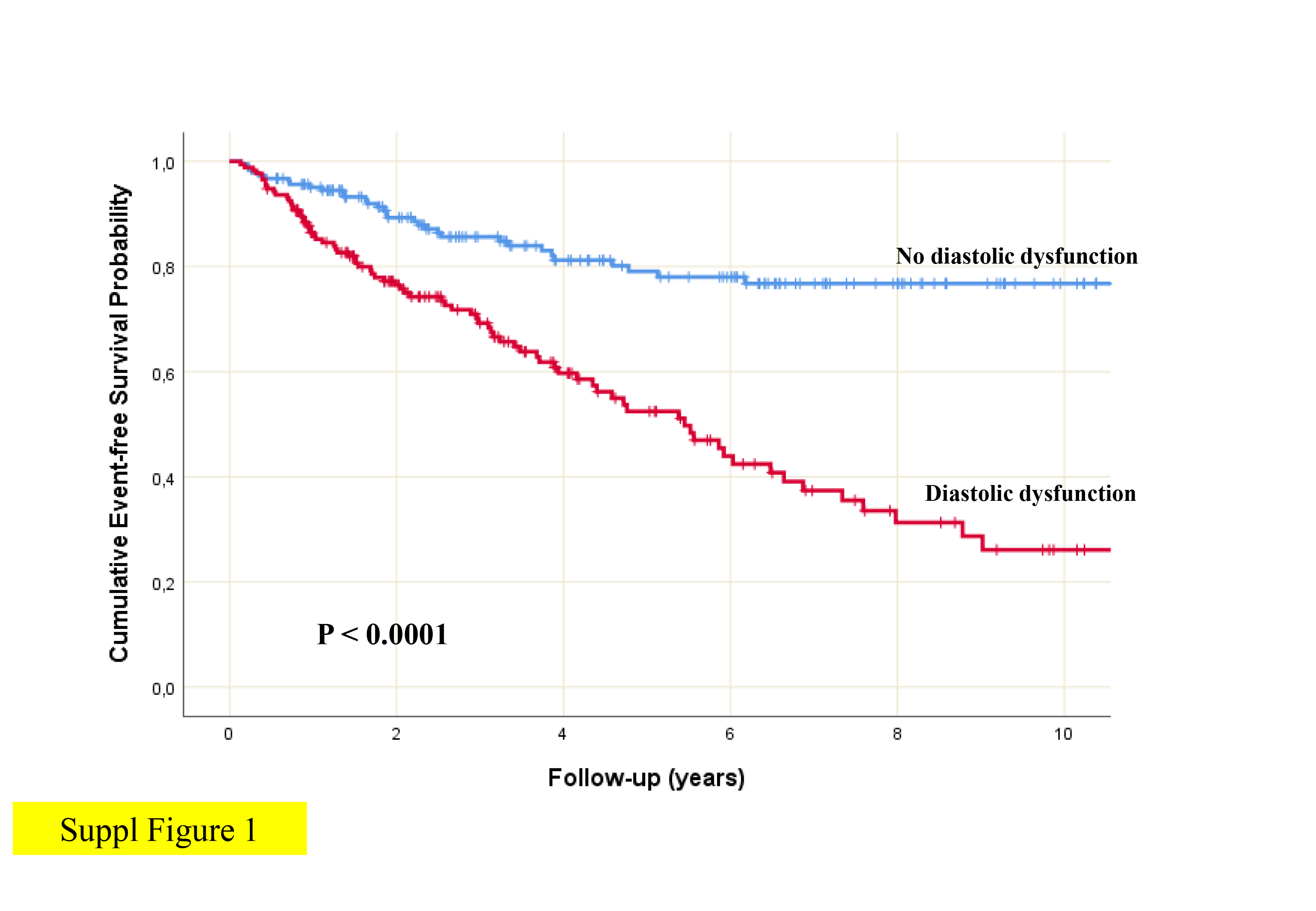
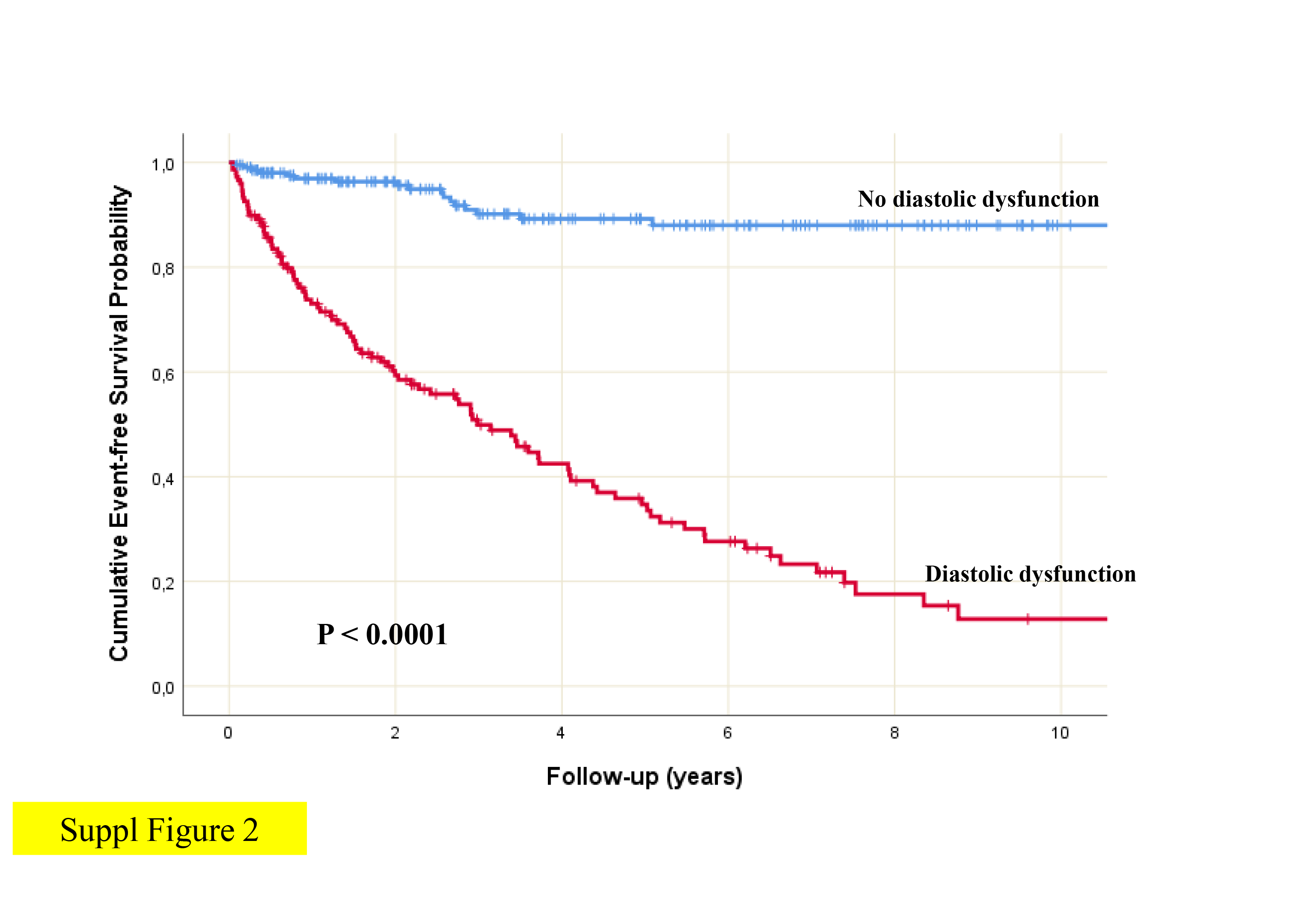
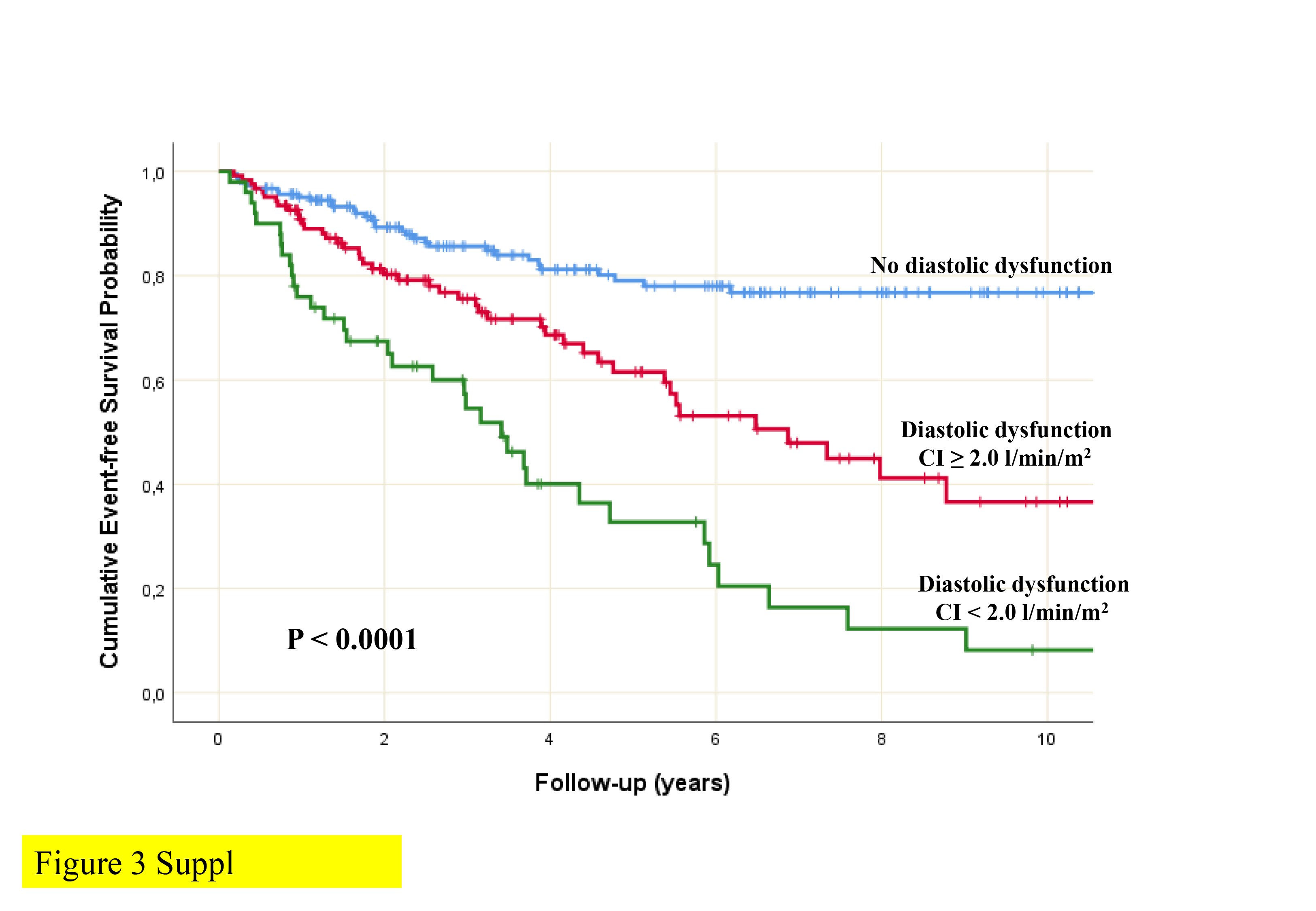
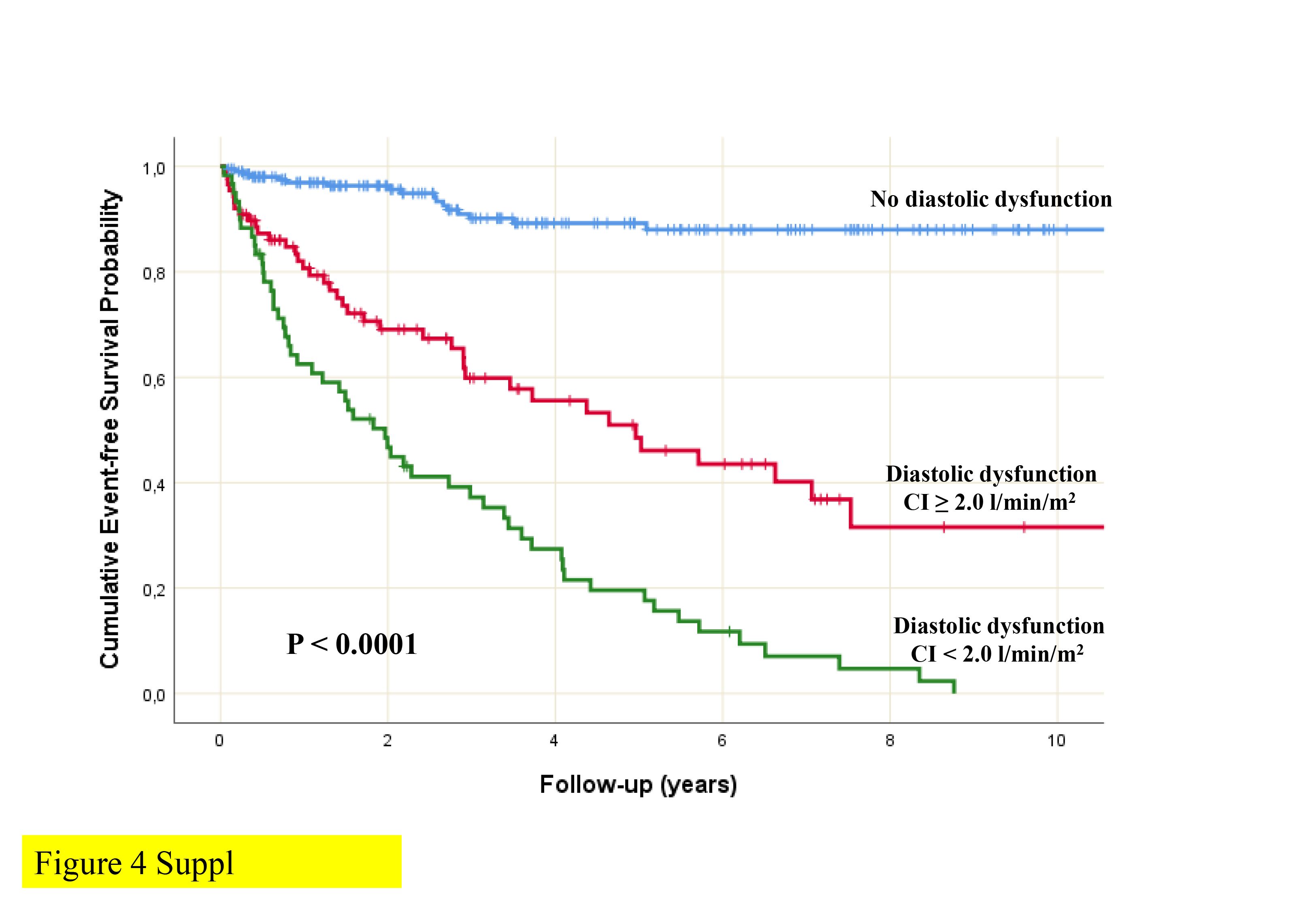
Echocardiographic hemodynamic classification. Study patients were classified according to the presence or absence of DD in the light of ASE-EACVI 2016 recommendations. Patients with elevated LVFP were considered those with E/A ≥ 2.0 or exhibiting > 50% of the following criteria: an average (of septal and lateral) E/e’>14, a septal e’<7 cm/c or lateral < 10 cm/s, a TRV > 2.8 m/s and a LAVi > 34 ml/m2. LVFP was considered normal if < 50% of previous criteria were present or when E/A ≤ 0.8 or E ≤ 50 cm/s. When ASE-EACVI 2016 recommendations could not determine DD, identification of elevated LVFP relied on an algorithm based on non-invasively measured pulmonary diastolic pressure[13]. Patients were defined as having normal forward flow if they had CI ≥ 2.0 l/min/m2, whilst a reduced forward flow was characterized by CI < 2.0 l/min/m2.[9]
Follow up. Patients were evaluated at baseline (index echocardiogram) and underwent clinical evaluation, BNP or NT-proBNP assessment and repeated echocardiographic examinations 6 ± 3 months afterwards. At follow-up, patients were classified into four groups based on changes in LV diastolic function: 1) persistently normal, if the diastolic function was normal on both baseline and follow-up exams; 2) reversible, if DD was present only at baseline; 3) worsening, if DD was present only at follow-up; 4) persistently abnormal, if the diastolic function was abnormal on both baseline and follow-up examinations. Abnormal natriuretic peptide concentration at follow-up was defined as BNP ≥ 150 pg / mL or NT-proBNP ≥ 450 pg / mL, along with failure to demonstrate ≥ 30% reduction from baseline[14].
Study endpoints. The endpoint was a composite of all-cause mortality and HF hospitalization. Survival data were obtained through follow-up visits of patients or, in the case of missed visits, through telephone contacts. Follow-up data were obtained by reviewing the patient's hospital records; death certificates were obtained in case of need. Survival analyses were performed considering the day of the follow-up examination as the starting day. For patients without events, the date of the last contact was considered the end of follow-up for survival analysis.
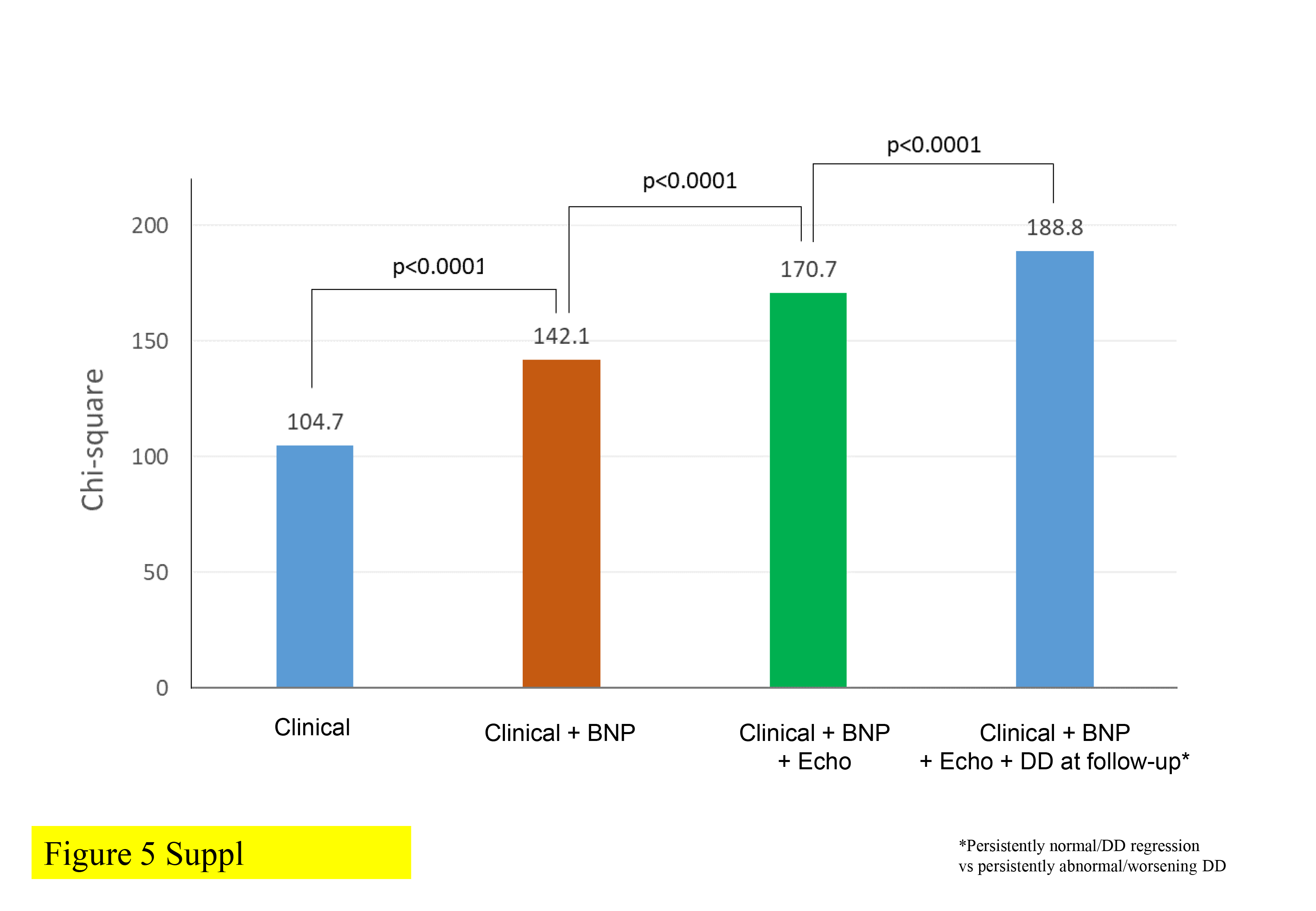
Statistical analysis. Data for continuous variables were presented as mean ± SD or as median with interquartile range in case of non-normal distribution. Categorical variables were presented as number and percentage. Differences in continuous variables among groups were analyzed by the Student's t-test or ANOVA, as appropriate. For non-parametric variables, the Mann-Whitney U test and the Kruskal–Wallis test were used. Categorical variables were compared by the Chi-square test or Fisher exact probability test when indicated. Two-way repeated-measures ANOVA was used to assess the effect of LV changes in LV diastolic function on CI. Kaplan-Meier curves were plotted to assess event-free survival probability across groups. Multivariate Cox proportional hazards regression was used to estimate the prognostic value of changes in LV diastolic function. Model discrimination was explored by receiver operating characteristic (ROC) analysis using the linear predictor score obtained from the proportional hazards model. The likelihood ratio test was considered to compare the performance among nested models and assess the incremental value of LV diastolic function changes over established predictors of outcome. Data were analyzed using the IBM SPSS Statistics software, v. 24. Differences were considered statistically significant for P < 0.05.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}