Demographic and baseline characteristics of the study population
The study flowchart is shown in Figure 1. Totally 614,355 patients were diagnosed with lung cancer during the study period; 11,341 of them met the eligibility criteria and were included in the current study. Slightly more than half (53.1%) of them were male. The upper lobes of the lungs were the most frequent primary site of NSCLC (53.4%); adenocarcinoma (54.3%) was the most common histological subtype of NSCLC. Furthermore, 56.3%, 38.5% and 5.3% of NSCLC cases had N1, N2 and N3 disease, respectively. The demographic and baseline characteristics of the study population are shown in Table 1.
CSS
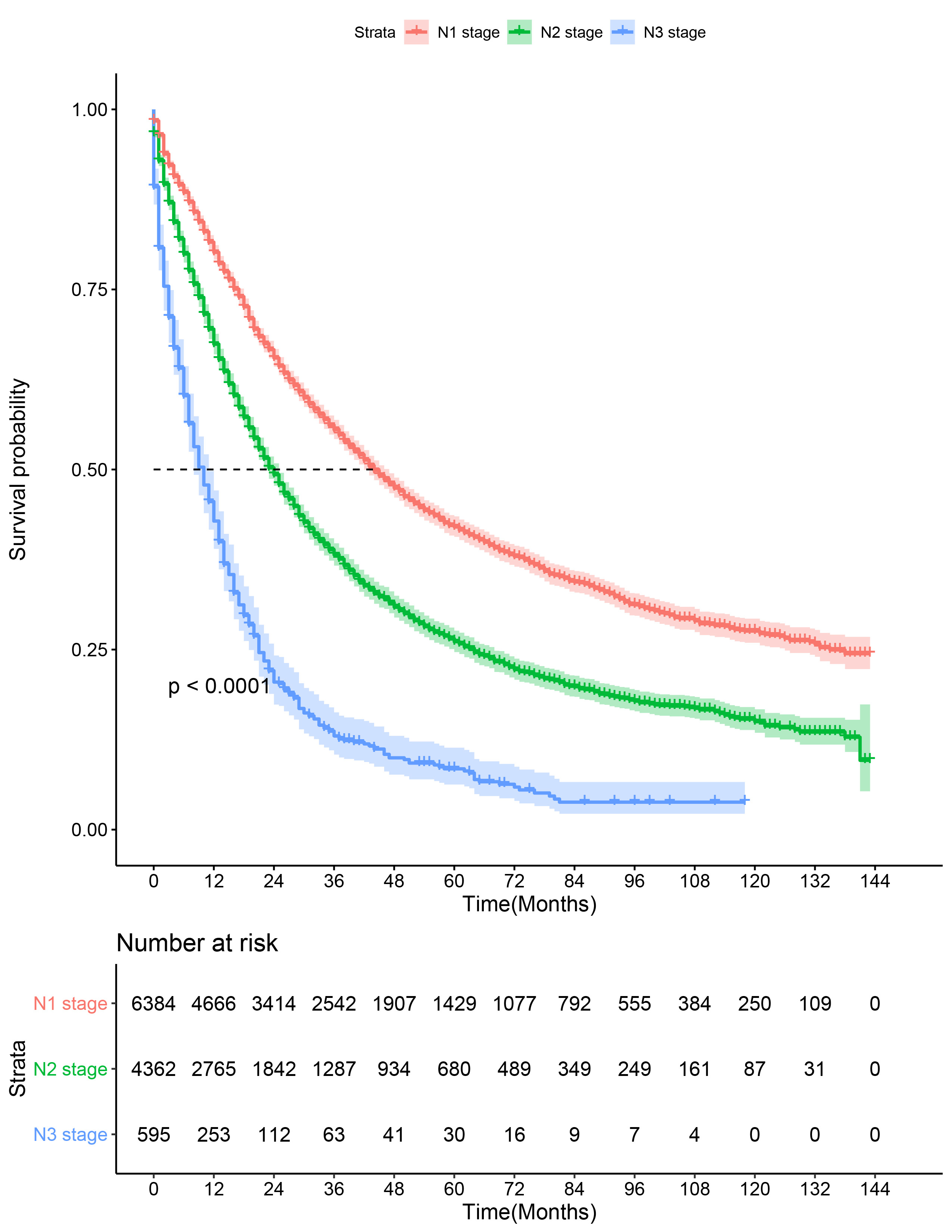
The patients were followed up for median duration of 22 months (Q1,Q3: 8, 48). Totally 5,757 patients died due to NSCLC during the follow up. The median CSS of the study population was 22 months (range 0,143). The median CSS of N1, N2 and N3 NSCLC cases was 26 months (range 0, 143), 19 months (range 0, 143), and 9 months (range 0, 143), respectively (Figure 2).
LNR and N stage
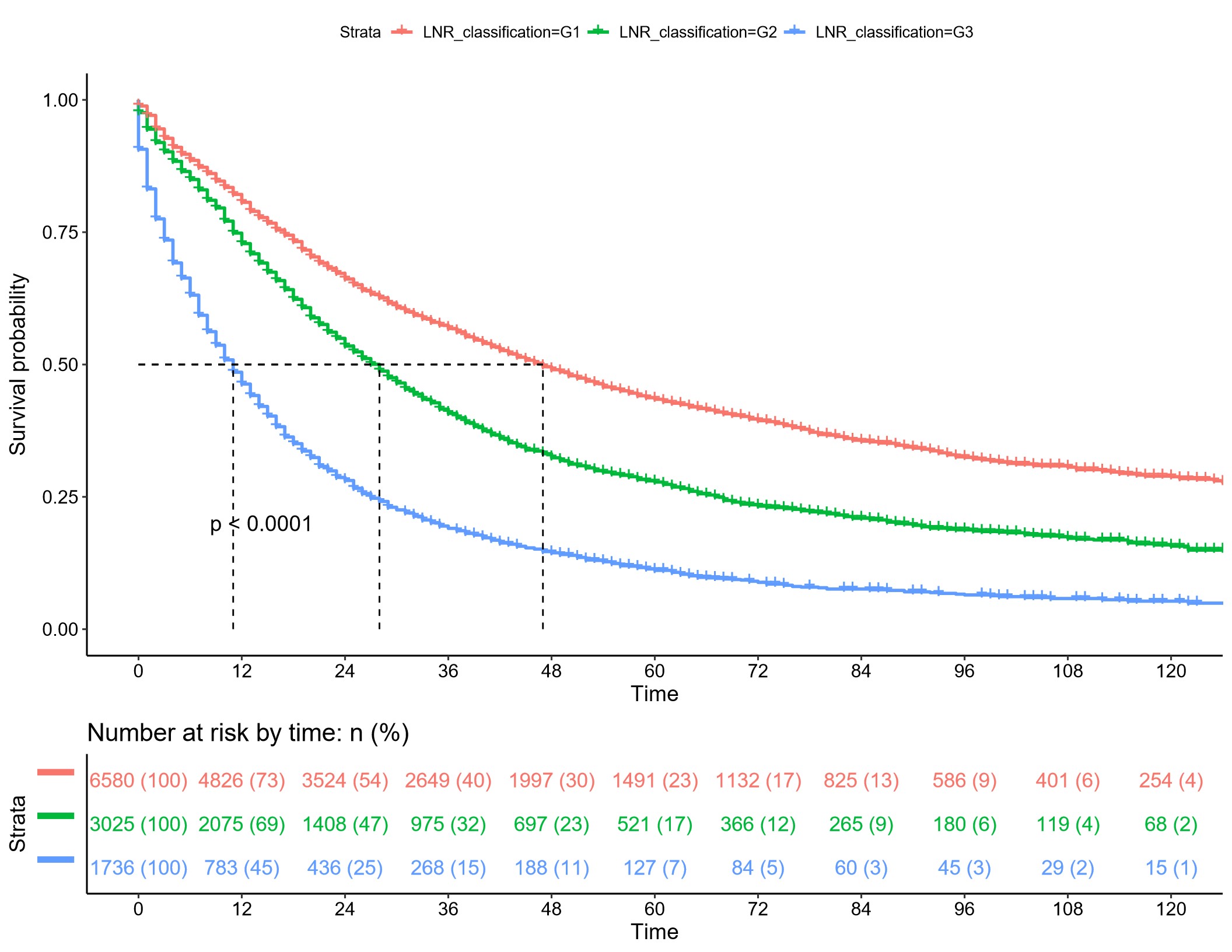
The median number of retrieved lymph nodes were 9 (Q1,Q3: 4,15) and the median number of positive retrieved lymph nodes were 2 (Q1,Q3: 1,3). The median LNR was 0.22 (Q1,Q3: 0.11, 0.50). X-tile analysis of CSS data of NSCLC cases from the SEER registry showed that the optimal LNR cut-off points were 0.28 and 0.81, which divided the entire cohort into low (LNR1 ≤ 0.28; n=6580, 58%), middle (0.28 < LNR2 < 0.81; n=3025, 26.7%), and high (LNR3 > 0.81; n=1736, 15.3%) subsets. Kaplan-Meier analysis further showed that patients with a low LNR had a significantly higher CCS versus patients with middle or high LNR (P< 0.001) (Figure 3A). Chi-square test showed a significant association of LNR with the median number of retrieved lymph nodes as well as the median number of positive and negative lymph nodes (P<0.001) and pT and pN stage (Chi-square test, P<0.001) (Supplementary Table 1). Our multivariate Cox regression analysis using LNR as a covariate further showed that higher LNR was an independent and significant adverse predictor of CSS (LNR3 vs. LNR1: HR: 2.73 95%CI 2.49, 2.99; P < 0.001) (Figure 3B).
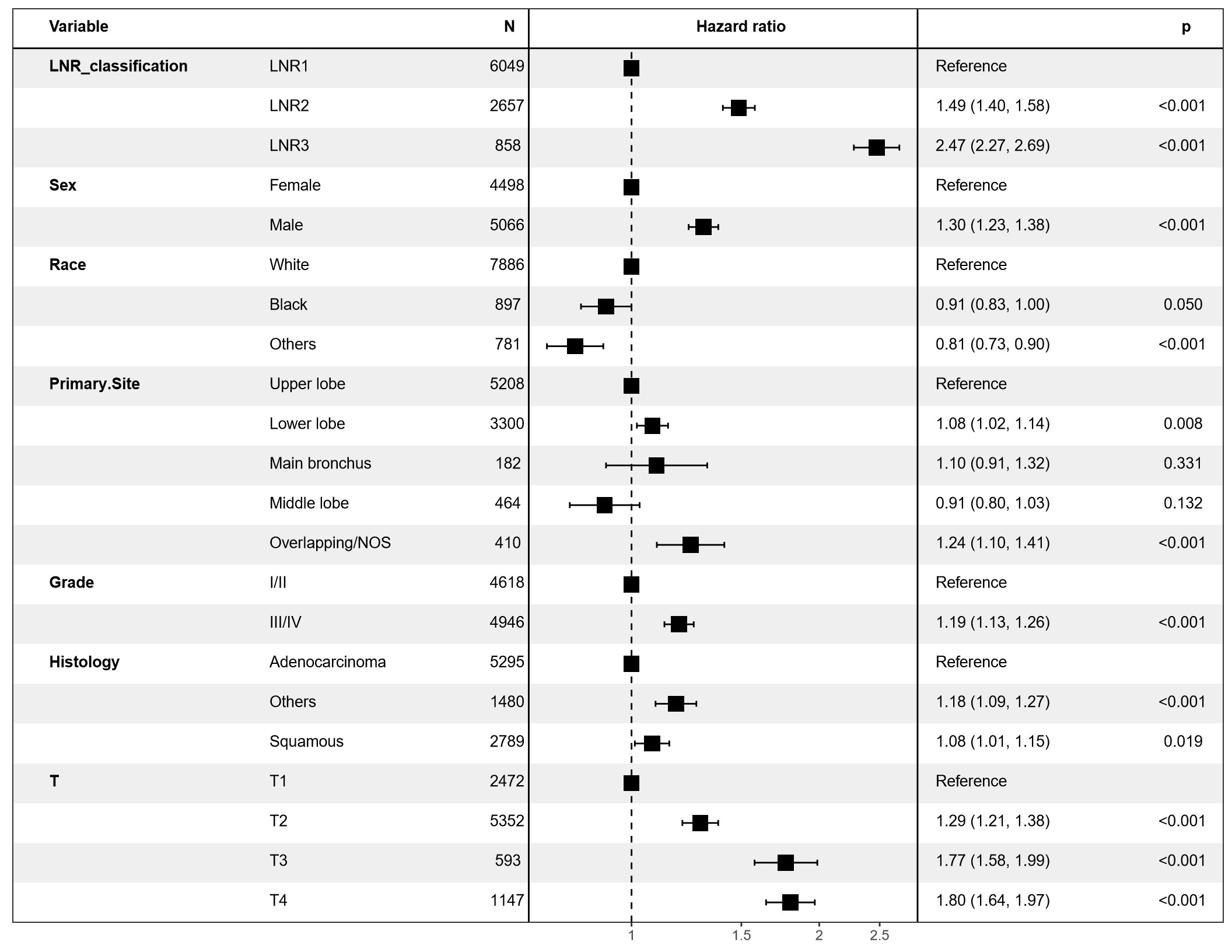
Our multivariable competing risks regression analysis, with inclusion of LNR and N stage, respectively, revealed that LNR was an independent and significant adverse predictor of CSS (LNR2 vs. LNR1: SHR: 1.56, 95%CI : 1.47,1.67, P < 0.001; LNR3 vs. LNR1: SHR: 2.54, 95%CI: 2.30,2.80, P<0.001) (Table 2). Moreover, our multivariate Cox regression analysis using pN as a covariate showed that higher pN was an independent and significant adverse predictor of CSS (N2 vs. N1: HR: 1.58, 95%CI 1.49, 1.68; P < 0.001 and N3 vs. N1: HR: 2.95, 95%CI 2.50, 3.49; P < 0.001) (Figure 3C). Furthermore, our multivariable competing risks regression analysis, with inclusion of LNR and N stage, respectively, revealed that pN was an independent and significant adverse predictor of CSS (N2 vs. N1: SHR: 1.54, 95%CI : 1.45,1.63, P < 0.001; N3 vs. N1: SHR: 2.81, 95%CI: 2.32,3.41,P < 0.001) (Table 2). Assessment of the two multivariate Cox models incorporating LNR and pN as covariates showed that LNR had a lower AIC value and was, hence, a better prognostic indicator of CSS than pN.
Prognostic stratification of pN diseases by LNR
We further sought to elucidate the relationship between LNR and pN stage as lymph node involvement is one of the most critical determinants of clinical outcomes and dictates treatment strategy of resectable NSCLC patients. A significantly greater proportion of patients whose LNR was ≤ 0.28 had N1 disease (LNR1 69.8% vs. LNR3:18.0%; P<0.001). Meanwhile, a significantly greater proportion of patients whose LNR was > 0.81 had N3 stage (LNR3: 26.8% vs. LNR1: 1.0% and LNR2: 2.1%; P<0.001).
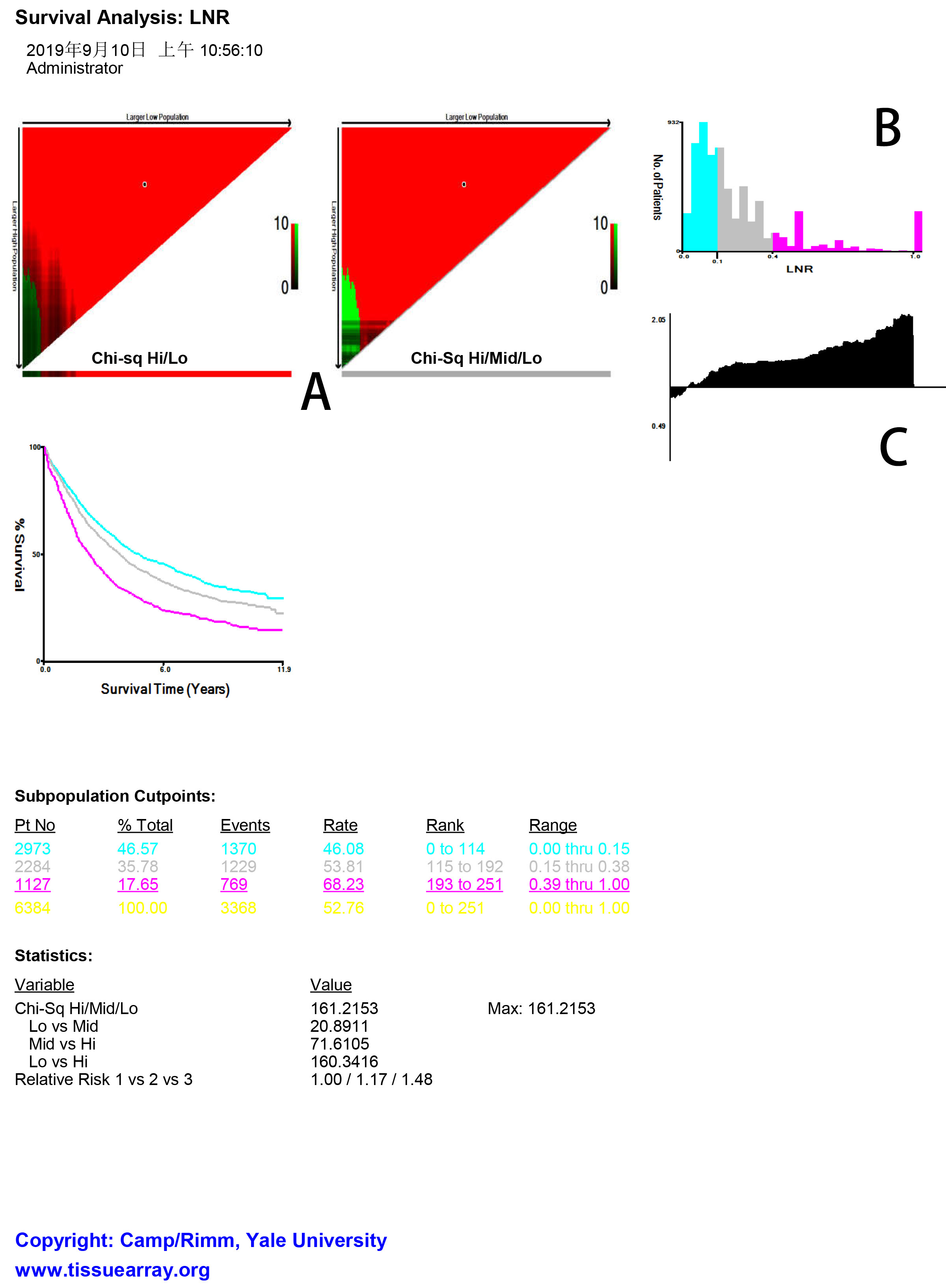
We then analyzed by X-tile the CSS data of N1 NSCLC cases and found that the optimal LNR cut-off points for the N1 NSCLC subpopulation were 0.17 and 0.38. The N1 subpopulation was divided by the two cut-off points into low (LNR1≤0.17; n=3425, 53.7%), middle (0.17<LNR2<0.38; n=1832, 28.7%), and high (LNR3>0.38; n=1127, 17.7%) subsets (Figure 4A). X-tile analysis of CCS data of N1 stage NSCLC cases from the SEER registry revealed a continuous distribution based on LNR (Figure 4A and B) and higher LNR was associated with higher RR (Figure 4C). Kaplan-Meier analysis further showed that patients with a low LNR had a significantly higher CCS (log rank test, P<0.001) (Figure 4D).
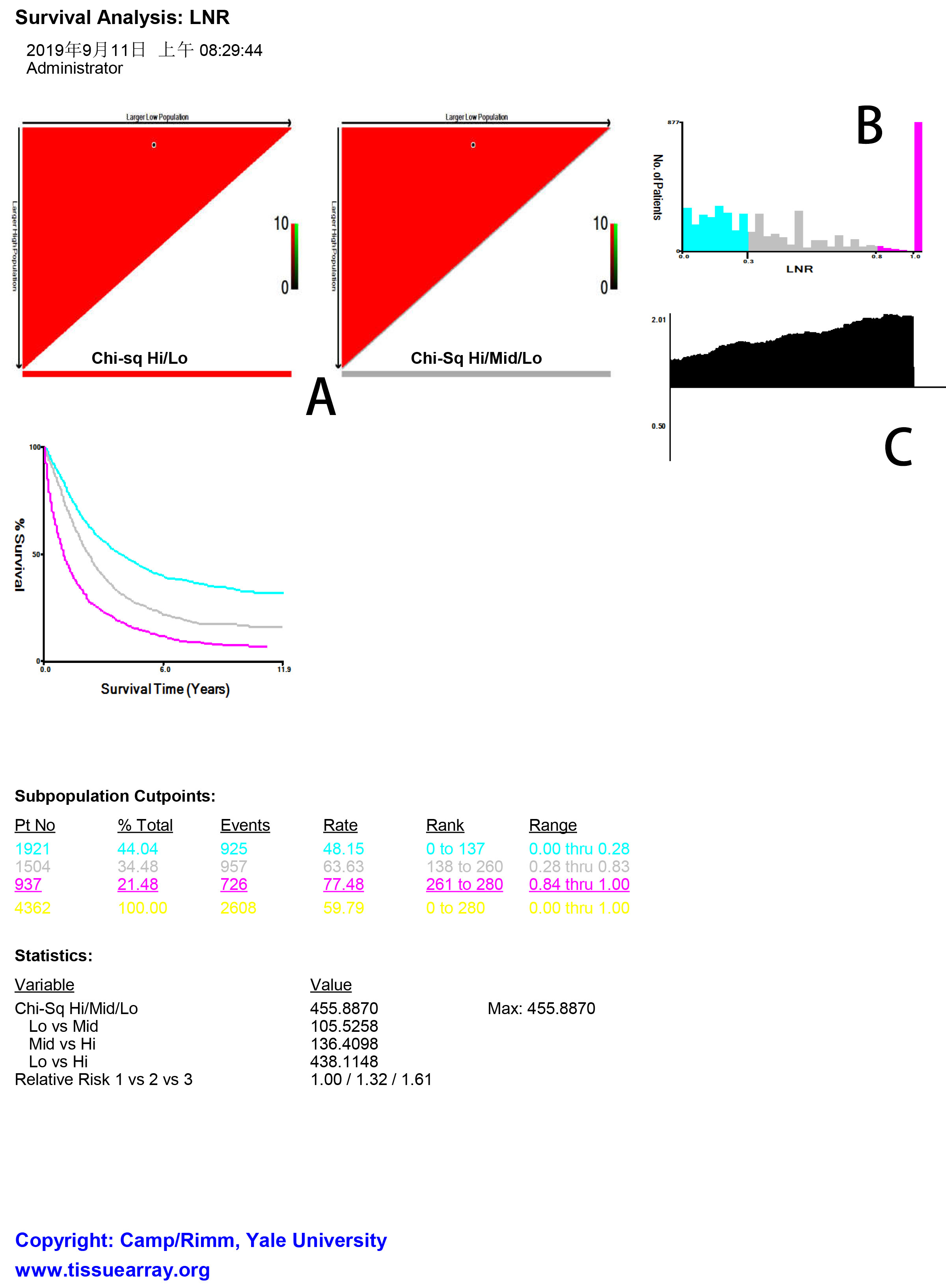
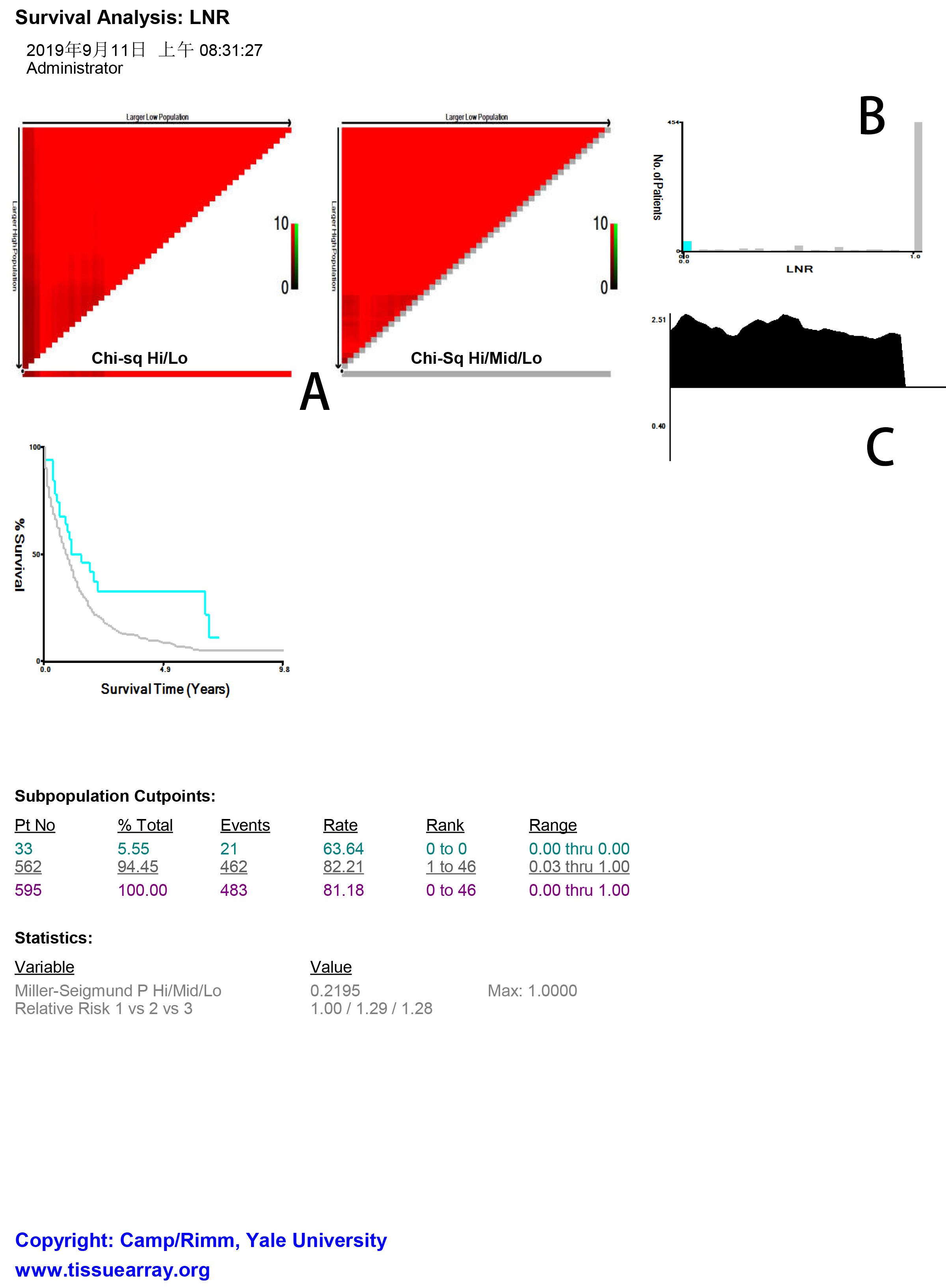
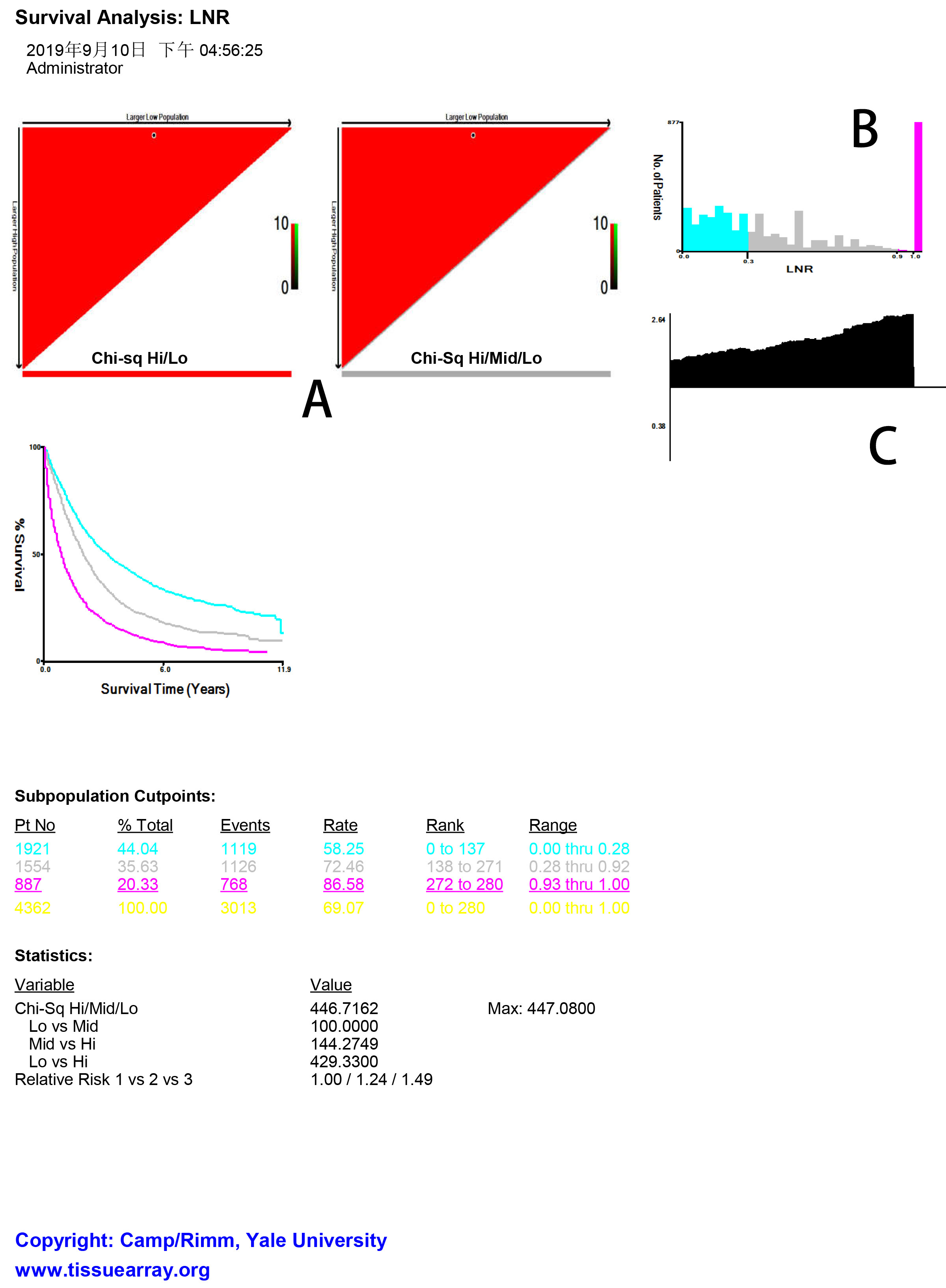
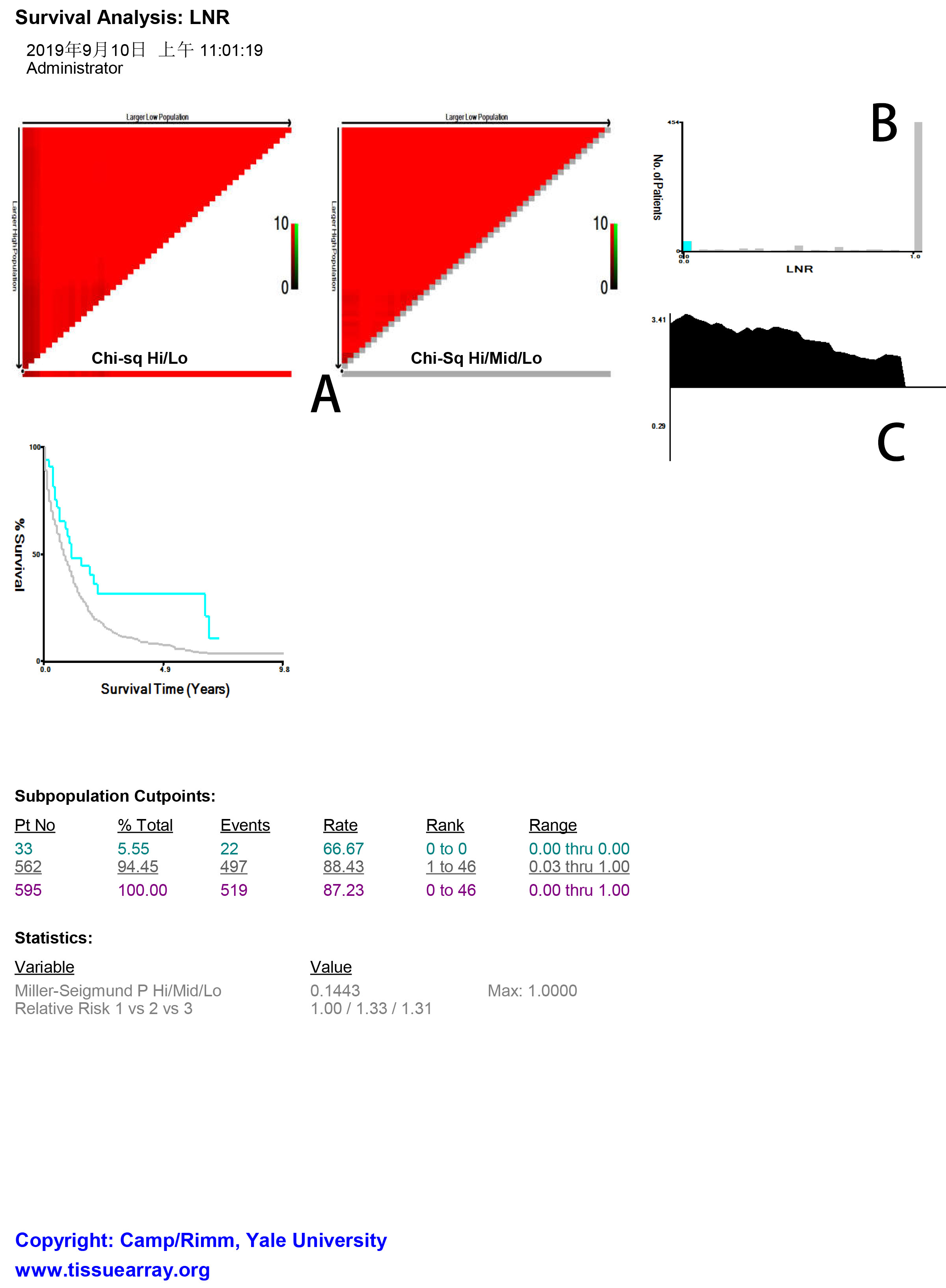
X-tile analysis of the CSS data of N2 NSCLC cases revealed that the optimal cut-off points of LNR for the N2 subpopulation were 0.30 and 0.80. The two cut-off points divided the N2 subpopulation into low (LNR1≤0.28; n=1921, 44.0%), middle (0.28<LNR2<0.83; n=1504, 34.5%), and high (LNR3 > 0.83; n=937, 21.5%) subsets (Supplementary Figure 1A to C). Kaplan-Meier analysis showed that patients with a low LNR had a significantly higher CCS versus patients with middle or high LNR (log rank test, P<0.001) (Figure 4E). Furthermore, X-tile analysis of the CSS data of N3 NSCLC cases showed that the optimal cut-off point of LNR for the N3 subpopulation was 0.03. The N3 subpopulation was categorized by the cut-off point into low (n=33, 5.6%) and high (n=562, 94.5%) subsets (Supplementary Figure 2A to C). Kaplan-Meier analysis further revealed that patients with a low LNR had a significantly higher CCS versus patients with high LNR (log rank test, P< 0.001) (Figure 4F).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}