We present a description of our experience of treating a rare condition, cystic neutrophilic granulomatous mastitis, in a tertiary infectious disease unit. Given the paucity of clinical data on this entity, this small retrospective study provides insight into our experience of clinical features, microbiological workup, treatment, and outcomes which will be valuable in similar settings.
Published antimicrobial treatment strategies for CNGM are diverse and founded on targeting lipophilic Corynebacteria. These have previously been based on in vitro sensitivities and therapeutic experience derived from the treatment of the much better characterised entity Idiopathic Granulomatous Mastitis (which is defined by the lack of an identified aetiological agent)[1, 3–6].
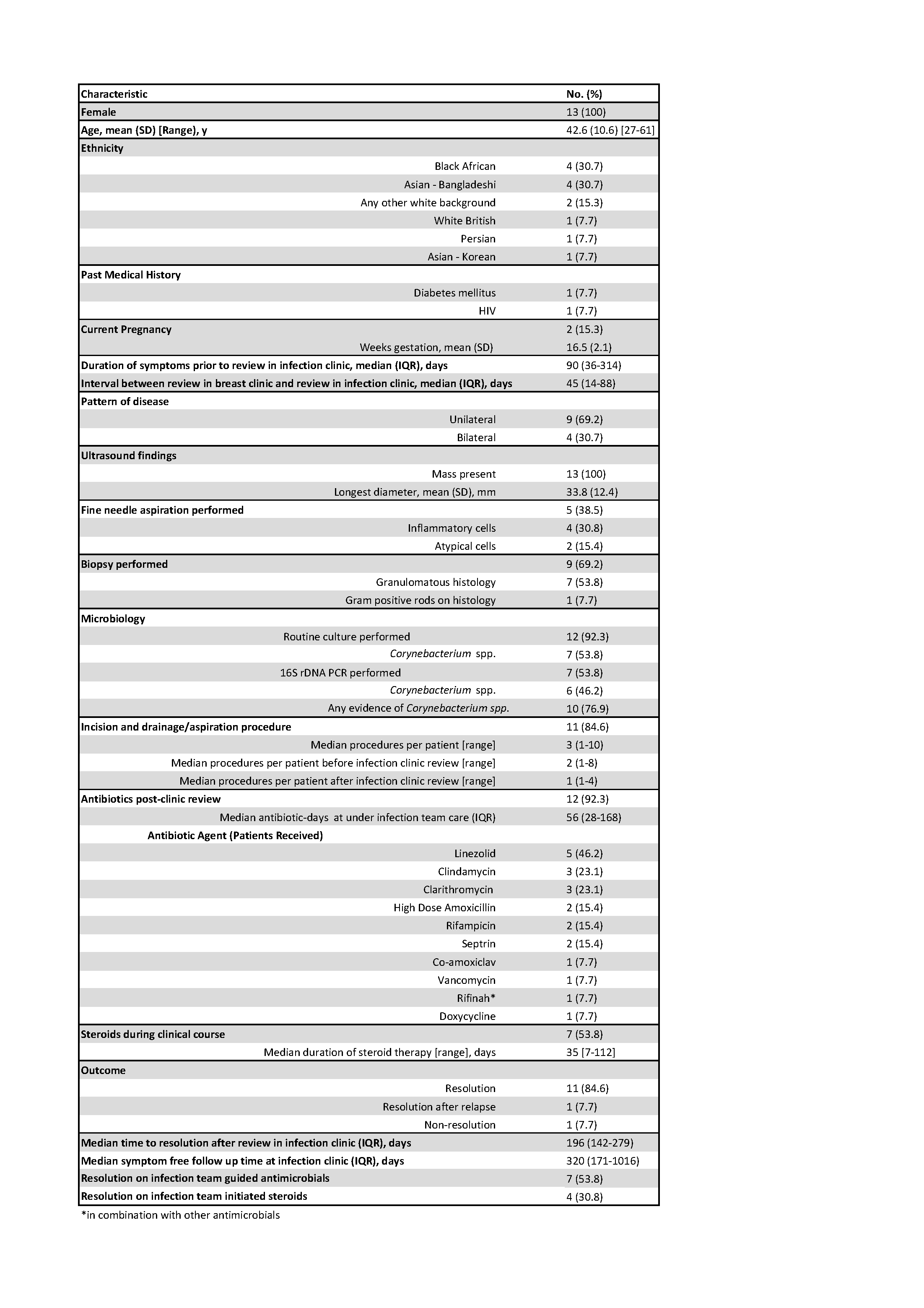
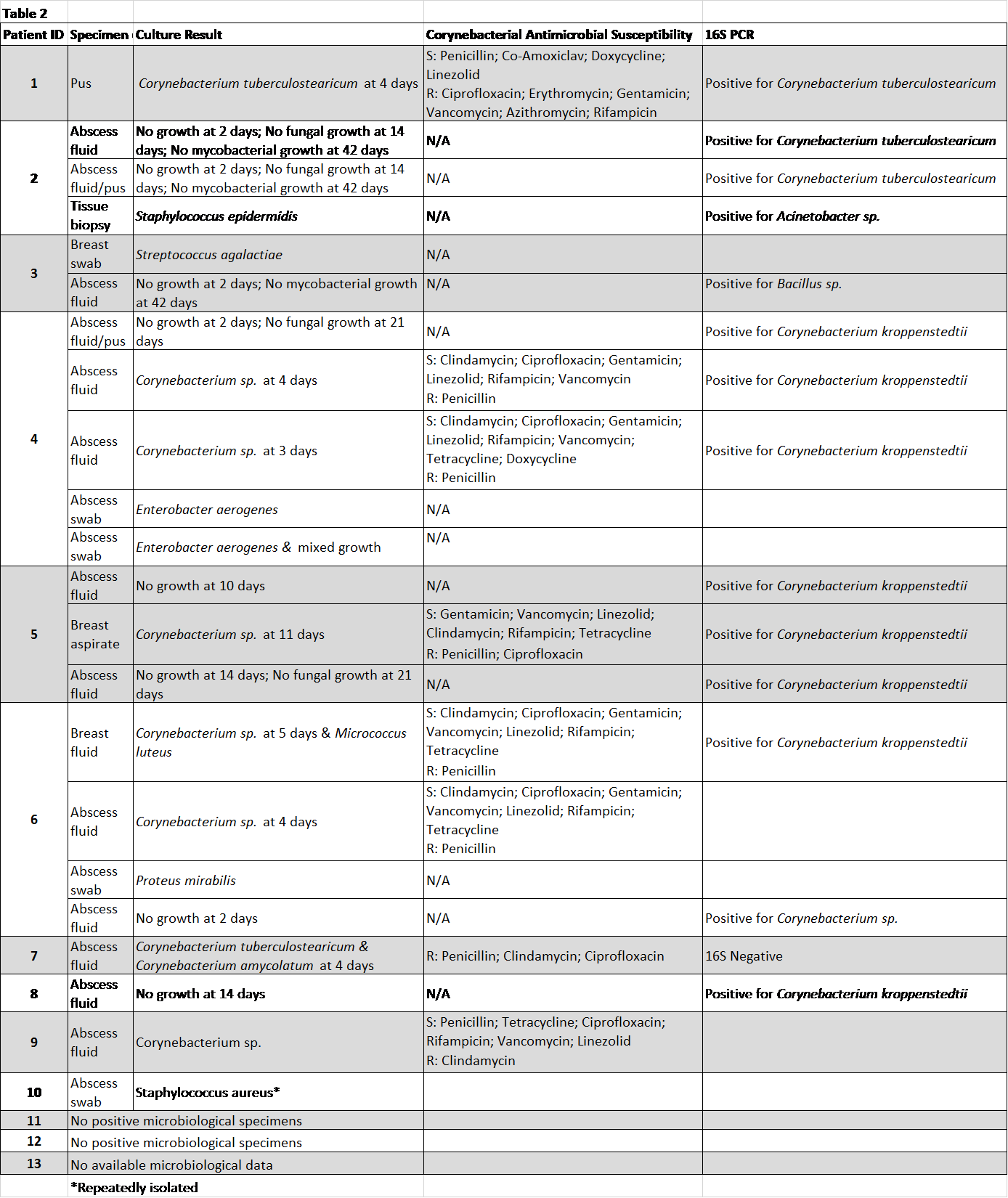
Lipophilic Corynebacteria such as C.kroppenstedtii, C.tuberculostearicum and C.amycolatum are fastidious organisms and frequently display broad resistance to standard antibiotic regimens[1, 9, 10]. Their exact role in the pathogenesis of CNGM is controversial; their presence may be co-incidental in areas of lipid rich inflammation (their preferred environment) or they may act as genuine contributors to pathogenesis in this context. However, it is interesting to note that broad-range 16S rDNA PCR was positive for Corynebacterium species DNA in 12/16 specimens (representing 6/8 patients tested) suggesting that routine use of such molecular assays may significantly increase the detection of these organisms. Commonly used antibiotics in this context include prolonged courses of agents such as Doxycycline, Vancomycin and newer drugs such as Dalbavancin[3, 5–7]. We demonstrate in our cohort a variety of antibiotic choices were viable, including Linezolid. Notably there were few reported side effects to antibiotic treatment, including Linezolid, in our cohort.
The relationship between CNGM and IGM is not well understood and a high degree of misdiagnosis and overlap is likely[1]. Treatment of IGM is variable between centres and includes conservative management, immunosuppressive therapy (in particular use of corticosteroids[11] and methotrexate[12]), and surgical excision of lesions and/or fistula tracts[1, 3, 7]. In general, the prognosis of IGM is good with complete remission in over 90% of patients treated with immunosuppressive therapies such as systemic steroids however time to recovery is often prolonged with median recovery times varying between 5 and 12 months[1, 3, 5, 7]. Our data on steroid usage mirror outcomes seen in the IGM literature and support ongoing use of immunosuppression as a treatment strategy in a significant proportion of patients.
The major limitation of this study is its small size and its retrospective nature. Additionally, we included four patients who had classical histology but no evidence of Corynebacteria, these patients may represent examples of disease on the GM spectrum rather than CNGM. Unfortunately, these obstacles are ubiquitous in previous reports due to the under-recognised and rare nature of the disease in addition to inconsistent classification and diagnostic criteria[1]. Further understanding of the optimal treatment for CNGM is unlikely to be achieved without the development of multicentre collaborations and we propose this should be a priority for future research.
Cystic neutrophilic granulomatous mastitis remains a challenging entity to diagnose and treat. Our centre has adopted a strategy of aggressive microbiological sampling (including 16S PCR) with targeted antibiotic treatment as first line therapy; supplemented by surgery and corticosteroids on a case-by-case basis. This approach has been mostly successful in our setting however optimal standardised treatment for CNGM remains elusive.
{kind=link}
{kind=link}