In the present study, statin showed primary and secondary preventive effects on cerebro-cardiovascular diseases in the 40–75-year-old adult group. However, only the primary preventive effect was statistically significant in the 60–75-year-old elderly group. Our findings elucidate that strict LDL-cholesterol control in elderly individuals aged 60–75 years is beneficial for the primary prevention of MACE.
The primary and secondary preventive effects of statin have been proven in previous studies. For primary prevention, Downs et al. showed a reduced risk for the first acute major coronary events in men and women aged 45–73 years, with average values for total cholesterol and LDL-cholesterol.22 Kim et al. specifically recruited 1,278 elderly individuals over 75 years to validate the effect of statin.23 Their study proved lower cardiovascular events and all-cause deaths with statin use, but the study was limited to participants from a single tertiary hospital. Kim et al. additionally used the National Health Insurance Services-Senior Cohort of 1,370 elderly patients over 75 years to demonstrate the primary prevention effect of statin in decreasing the all-cause mortality if statin was used for at least 5 years.24 Our study similarly showed the primary preventive effect of statin. However, it differed in that we used the nationwide health screening cohort data, which included a broader age range and a greater number of elderly individuals.
The Heart Protection Study (HPS)25, Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 trial (PROVE-IT)26 and Reversal of Atherosclerosis with Aggressive Lipid Lowering studies27, all demonstrated the secondary effect of statin in preventing MACE among patients with accompanying coronary diseases, occlusive arterial diseases, or diabetes.
Another important drugs to prevent cardiovascular events are aspirin and clopidogrel. In secondary prevention trials of aspirin, the potential benefits of reducing the occurrence of MACE were significant and outweighed the potential risk of hemorrhages.13–15 In primary prevention trials, however, aspirin did not show an effect on MACE. In the Aspirin to Reduce Risk of Initial Vascular Events trial28, aspirin showed no effect on MACE in adults with multiple risk factors for cardiovascular diseases but showed increased gastrointestinal bleeding. In the Aspirin in Reducing Events in the Elderly trial29, aspirin was randomly assigned to the patient group who were 70 years or older, but the study was terminated early for futility. Aspirin had no effect on disability-free survival but significantly increased the risk of major hemorrhage and all-cause mortality.
Similar to aspirin, the secondary preventive effect of clopidogrel is proved through multiple studies. Bhatt et al. showed lower MACE with clopidogrel compared to the placebo group.16 Moreover, this benefit was more pronounced in patients with prior MI or ischemic stroke than peripheral artery disease. In the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) study30, however, the primary preventive effect of MACE by clopidogrel was not statistically significant; what is more, a higher risk of severe bleeding was seen in the primary prevention group compared with the secondary prevention group. Currently, no studies have demonstrated the primary preventive effect of aspirin and clopidogrel on CVDs.
In comparison to aspirin and clopidogrel, statin showed both primary and secondary preventive effects on CVDs. Moreover, continued lowering of LDL-cholesterol through statin use is recommended in the elder group over 60 years old. Sabatine et al. even suggested that further lowering of LDL-cholesterol can further reduce cardiovascular risks.31 Other studies, such as HPS and PROVE-IT, suggested continued lowering of LDL-cholesterol to levels substantially below current guideline recommendations, regardless of the initial LDL-cholesterol concentrations.25–26
We focused on the elder group due to the less stringent treatment goals in elderly individuals with other cardiovascular risk factors, such as hypertension and diabetes. Until Beckett et al. published the Hypertension in the Very Elderly Trial32, epidemiologic studies pointed to the inverse relationship between blood pressure and the risk of death among people over 80 years old, thus possibly reflecting the increased risks of strict blood pressure control. For diabetes control, hemoglobin A1c, blood glucose levels, cognitive function, life expectancy, functional impairments, polypharmacy, nutritional defects, and other factors for overall health care must be all considered for the diabetic elderly people over 65 years old.10–12 Since the timeline of benefit is estimated to be at least 8 years for glycemic control11, the decision to treat diabetes should be based on the benefit and risk ratio for everyone concerned. Gerstein et al. even demonstrated excessive deaths with intensive glucose control in the elderly while MACE was not significantly reduced.33
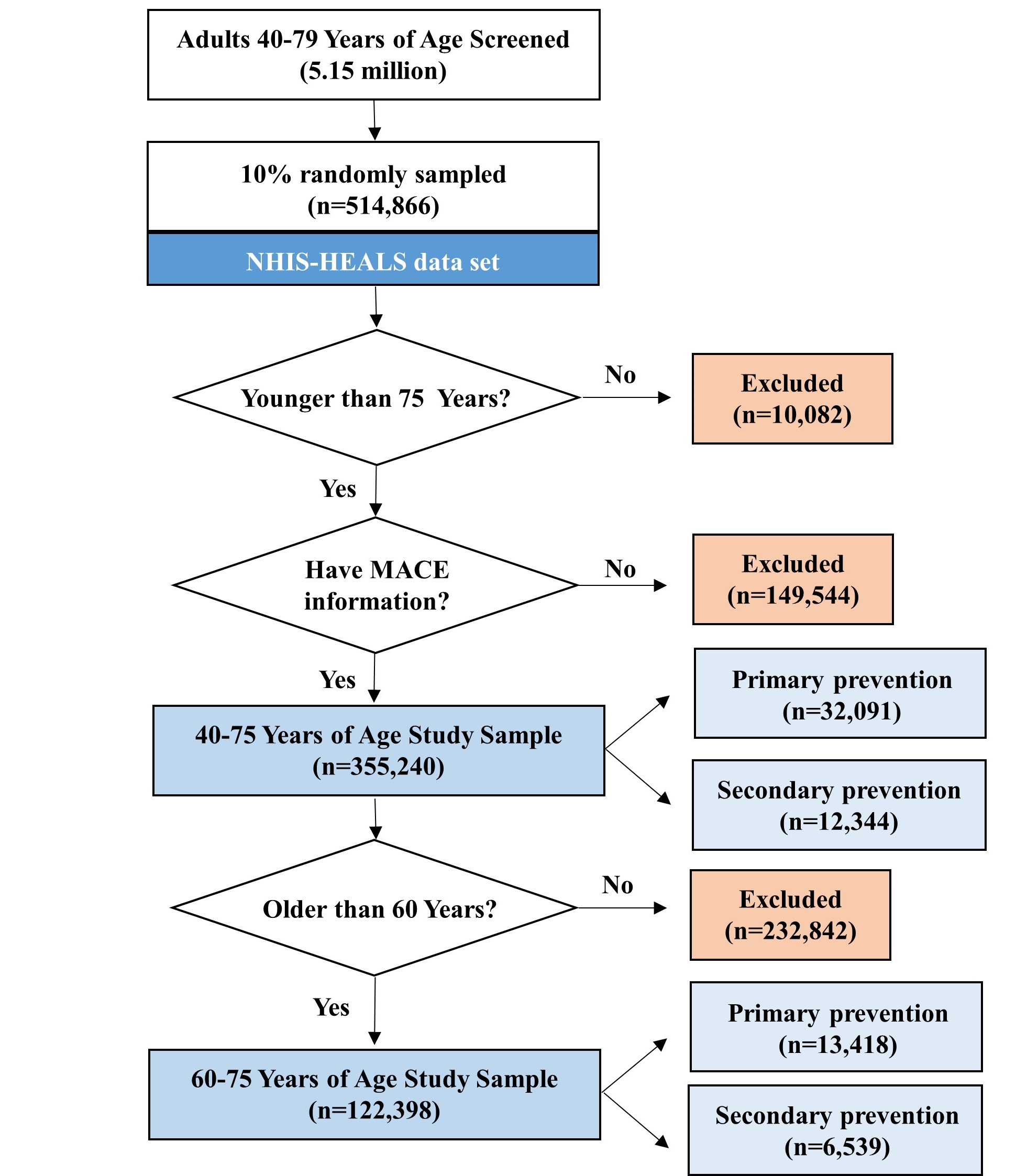
Previous studies using the 2013 ACC-AHA guidelines showed an improved CVD prediction and called for increased statin eligibility among elderly and diabetic patients.8,20,34 Baigent et al. conducted a meta-analysis showing further LDL-cholesterol reduction has a definite effect of reducing the incidence of heart attack and ischemic stroke.35 Therefore, our study investigated and proved the primary and secondary effects of statin in preventing cardiovascular diseases among adults from not only the total population of 40–75 year-olds but also the elderly group of 60–75 year-olds. Since a set LDL-cholesterol threshold is controversial and asymptomatic atherosclerosis begins during childhood36, future studies are needed to consider early statin use or to recommend strict LDL-cholesterol reference when a patient has risk factors for CVDs.
This study was subject to a few limitations. Administration of drugs that may affect the incidence of MACE, such as aspirin and clopidogrel, has not been investigated. Since antiplatelets and anticoagulants can function as confounding variables, it is necessary to control medications in the study. Furthermore, the mean follow-up duration was limited to 4.6 years due to LDL-cholesterol data availability. Longer follow up period is critical to determine the severity of MACE.
{kind=link}