Study Design:
This study was approved by the Anesthesiology and Pain Research Center, Ahvaz Jundishapur University of Medical Sciences (PAIN-9805), under the supervision of the AJUMS Research Ethical Committee (IR.AJUMS.REC.1398.097). This study was accomplished at the Cardiac Surgery unit of Golestan Hospital. Ahvaz. Iran between February and September 2019. After the approval of the ethics committee of Ahvaz Jundishapur University of Medical Sciences, Written informed consent was collected from the patients. All procedures performed according to the standard of care of the center. Inclusion criteria were: Age of patient between 30 to 75 years, candidate for on-pump cardiac surgery. Exclusion criteria were: a history of renal disease, BMI>35, EF<30%, drug history that directly affects the kidneys like NSAID, electrolytes disturbance, urgent surgery, redo surgery.
CSA-AKI diagnosis was based on KDIGO criteria, (ie, an increase in SCr by ≥0.3 mg/dL or greater within 48 hours; or an increase in SCr to≥1.5 times baseline, within 7 days after surgery) (2).
After arrival at the operation room, standard monitoring including five-lead electrocardiography, pulse oximetry, and arterial line for continuous blood pressure monitoring and blood gases were inserted. The sensors of NIRS were connected on the right and left flank area. Before the induction of anesthesia, kSo2 was recorded as a baseline. A standard anesthesia technique was used for all patients. After induction of general anesthesia, a central venous catheter was introduced. For initiation of cardiopulmonary bypass, 350 u/kg of heparin was injected for each patient. Heparin dosage was attuned based on goal ACT 450-480 second. CPB time and cross-clamp time were recorded. After the CPB was terminated, protamine (1mg/kg) was given for the reversal of heparin. CPB , cardiac surgery and postoperative management were standardized for all patients.
After surgery, all the patients were admitted to the cardiovascular ICU, with a standard protocol for sedation, analgesia (propofol 0.5 mg/kg/h and morphine sulfate 0.1 mg/kg/h), and management of mechanical ventilation (SIMV mode of ventilation). They were extubated when to found weaning criteria.
Study Patient:
148 patients were enrolled to study and according to inclusion criteria 107 patients were selected for analysis, and 41 patients were excluded and of them, 107 patients completed the study. In follow up stage 6 patient was excluded owing to lack of information and finally, 101patients were investigated. Consort diagram
Study Variables and measurements:
Demographic data included age, sex, body mass index, history of diabetes mellitus, hypertension, left ventricle ejection fraction, Euro SCORE, kidney depth, baseline kSo2, preoperative hemoglobin, preoperative SCr, and estimated glomerular filtration rate. Laboratory postoperative parameters were collected during the following stages of the study: ICU admission, 6 hours, 12 hours, 24 hours, and 48 hours postoperatively. The arterial blood gas analysis was measured for all of the measurement points (T0-T48).
The primary outcomewas: postoperative CSA-AKI defined by the KIDGO criteria.
The secondary outcomesincluded: cardiac and non-cardiac complications, such as circulatory arrest, reoperation, sepsis, low cardiac output (cardiac index less than 2.2 mL/min/m2), pneumonia, hepatic dysfunction, prolonged mechanical ventilation time (PMV: mechanical ventilation time >48 hours), massive transfusion (need to >10 units of blood component), mortality, need to RRT (renal replacement therapy), length of ICU stay.
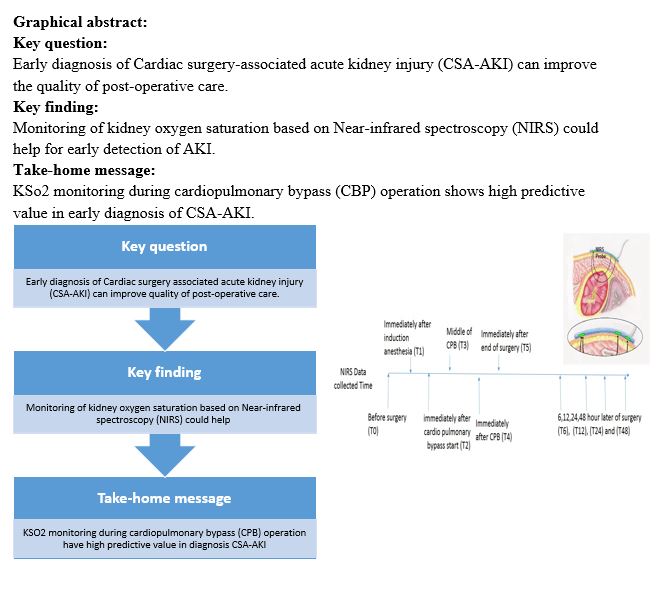
The time points of measurement of kSo2 were: before surgery (T0), immediately after induction of anesthesia (T1), immediately after starting of cardiopulmonary bypass (CPB) (T2), during CPB (T3), immediately after weaning of CPB (T4), immediately ICU admission (T5). Left and right Kidney saturation were measured in T0-T5 by NIRS (INVOS 5100C; Medtronic, Inc, Minneapolis, Minn).
We assess the correlation between kSo2 records with CSA-AKI using the KIDGO criteria (13).
Statistical Analysis:
The normality of all data was checked by Kolmogorov-Smirnov (K-S), Shapiro-Wilk test, D'Agostino skewness test (14). The parametric and non-parametric correlation was calculated for all analysis variables to each other. The sensitivity and specificity of kSo2 were analyzed by AUC-ROC analysis. Time course DATA was analyzed by RM-ANOVA and non-parametric RM analysis. The frequency of secondary outcomes was examined by the Fisher exact test.
{kind=link}