One of the reasons why we still have not yet identified a unifying, underlying reason for shunt failure is because of the unique positioning of shunt systems. They are inserted through cerebral cortex into the cerebral ventricles then bathed in CSF, where the shunt catheter is subject to protein adsorption, cells, tissues, and cellular debris with unknown variances in degree. Excluding shunt systems which fail due to distal effects such as displacement, disconnection, or valve disfunction, it is easy to imagine CSF shunt systems which fail must have failed in relationship to the factors present in the patient CSF. Previous evidence suggests elevated pro-inflammatory cytokine levels in CSF are conducive to worsening clinical outcomes in neuroinflammatory diseases26–28. However, to date there is no comprehensive hydrocephalus-focused CSF collection project focused on shunting and shunt failure and their relationship with neuroinflammation. Many cases of shunt failure are captured emergently or during off-peak hours, meaning routine CSF capture by research personnel may be expensive or have a latency in capture speed. The work presented here yields preliminary data to guide the direction of future experiments by shedding light on the expression profile of cytokines and MMPs in patient CSF immediately prior to revision surgeries.
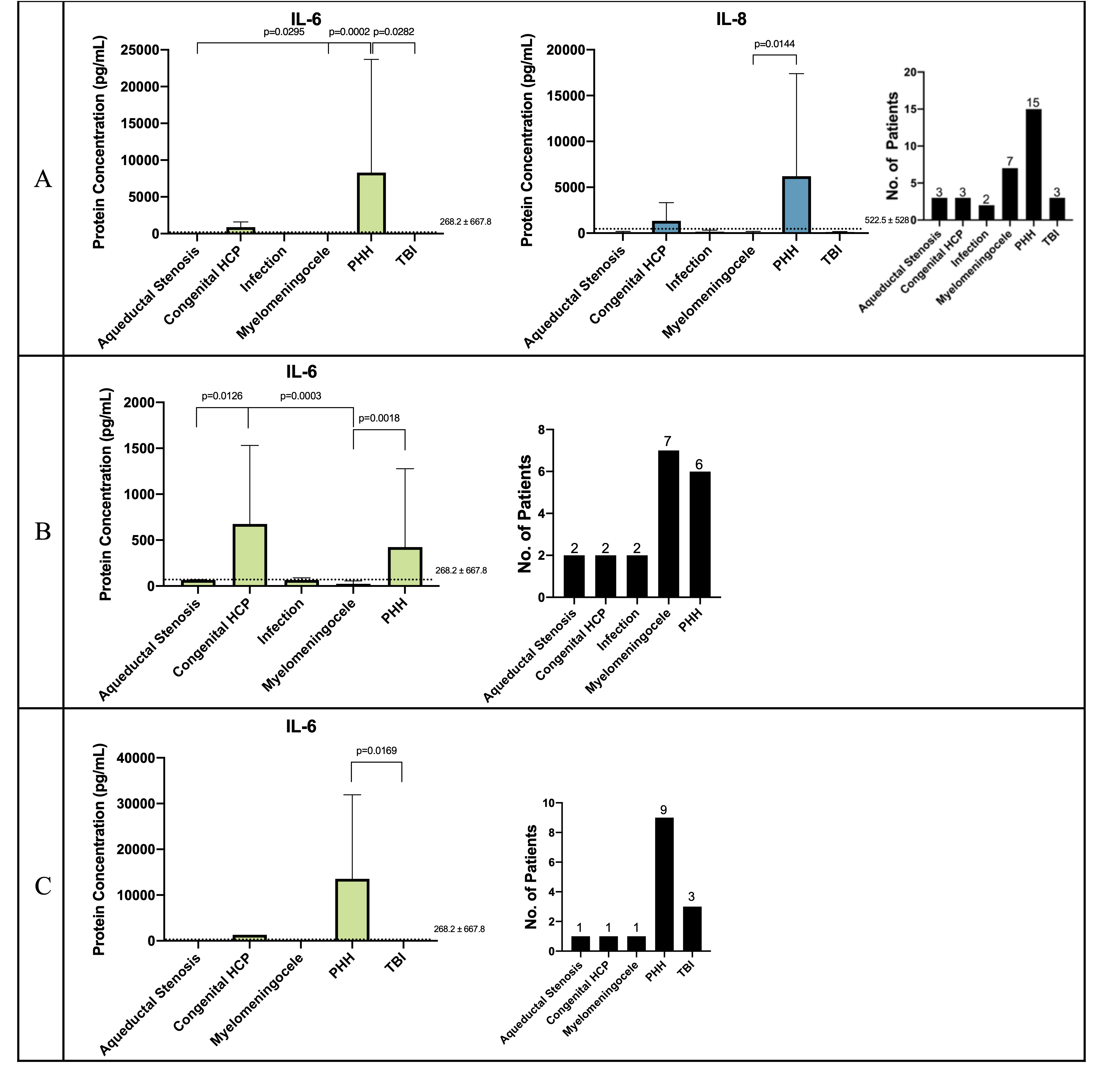
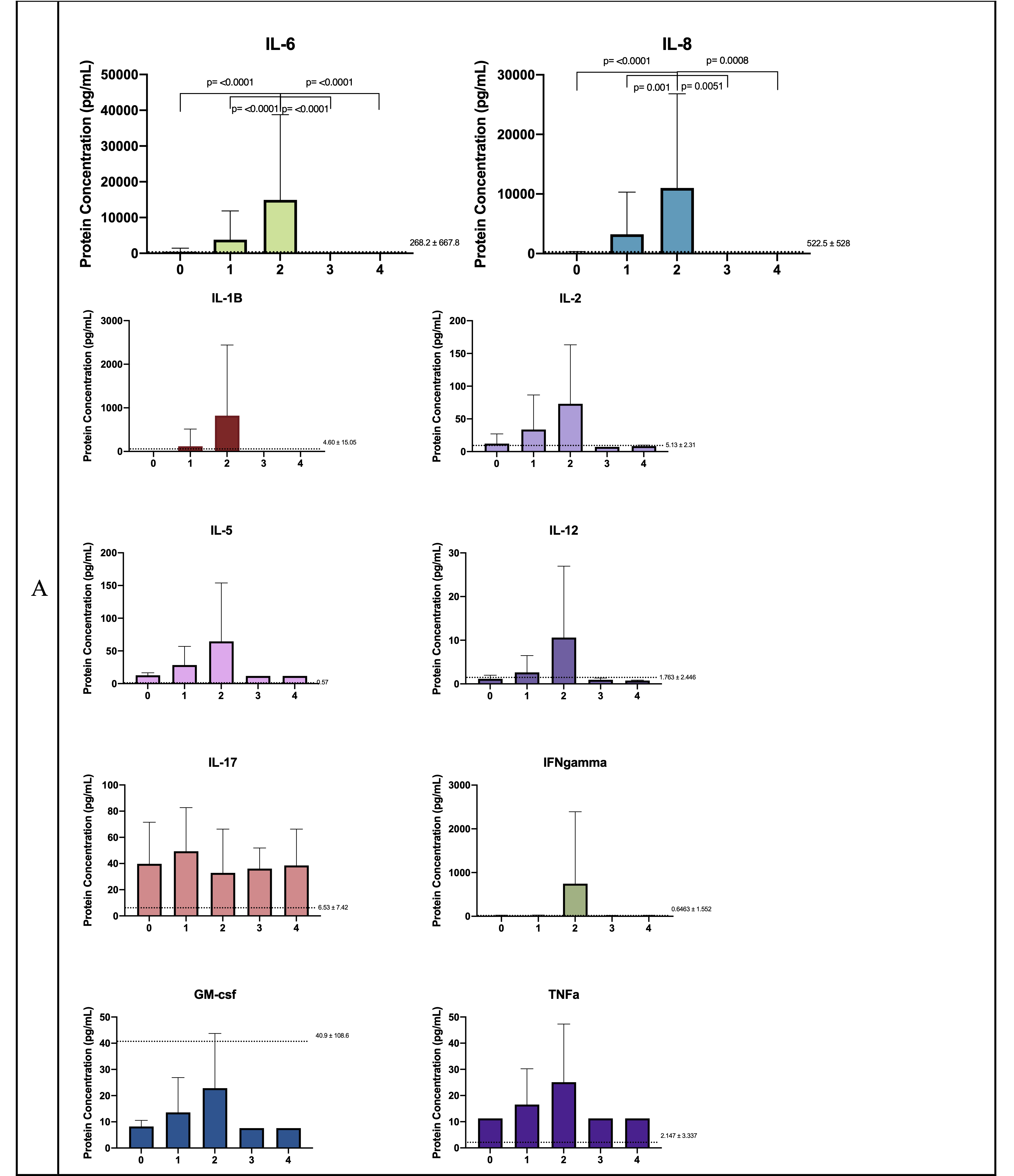
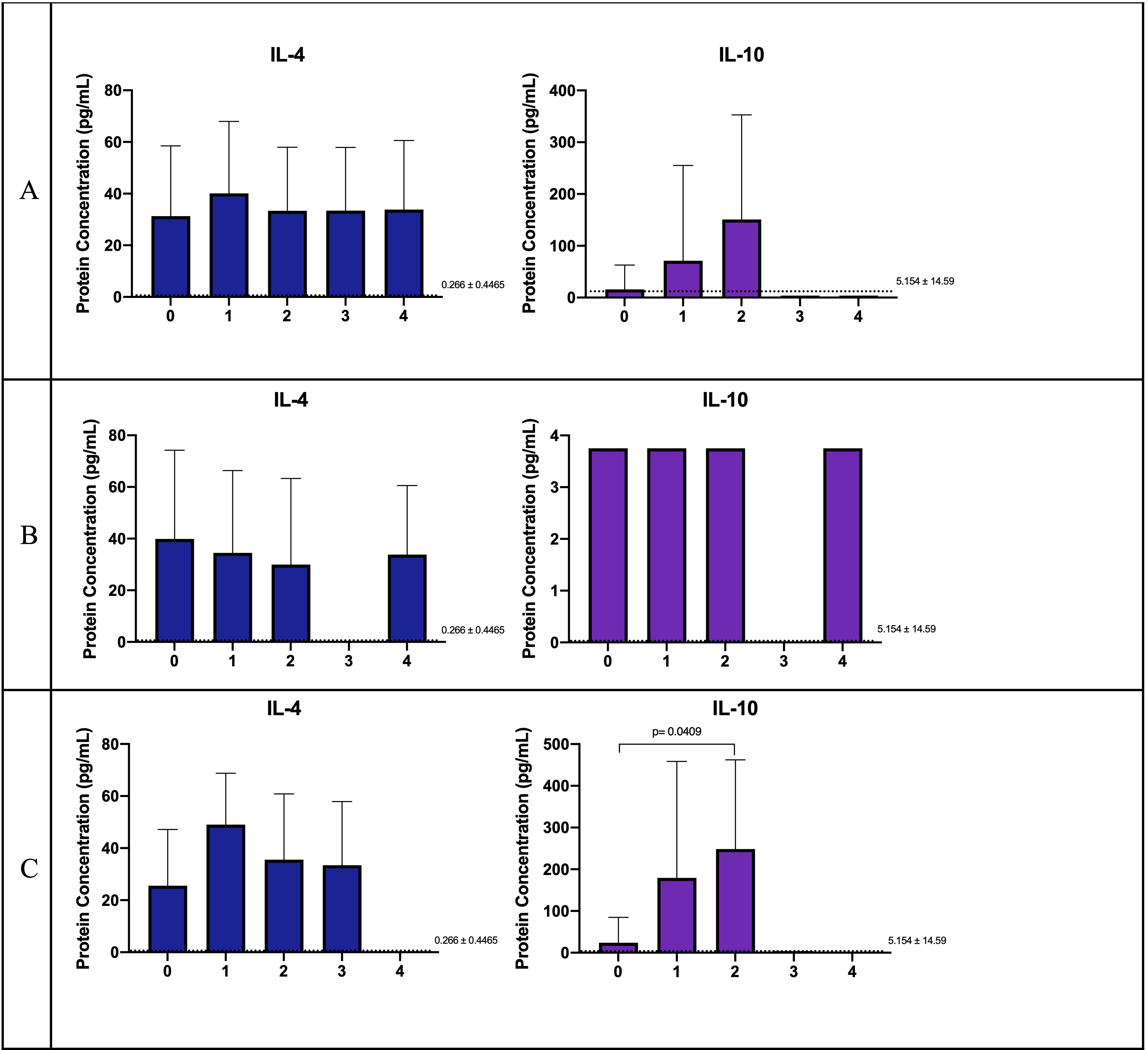
By looking at protein concentration levels, our results for the analytes tested suggest cytokine expression and MMP activation is generally decreased or within error in individuals with revised shunts due to symptoms of obstruction compared with those that failed for non-obstructed reasons (Fig. 3-Figure 8, supplementary Figs. 1–4). Meaning, that despite most of the pro-inflammatory cytokines and MMPs protein concentrations being close to healthy control levels or within deviation between obstructed and non-obstructed cases, other major cytokines and select MMPs stand out and consistently. These analytes with significant increase in non-obstructed cases at total protein concentration levels are IL-10, IL-6, IL-8, and MMP-7. Low sample size may preclude this as a predictor, however. Inclusion of referenced healthy controls as baseline shows the protein concentration levels for almost all of the cytokines and MMPs tested are either elevated or at baseline in all of the dependencies examined (Figs. 4–7).
Sorting by etiology reveals IL-6 as significantly increased in both obstructed and non-obstructed individuals and primarily for PHH and congenital HCP patients, while IL-8 is significantly higher in PHH patients when all of the data is considered. The lack of significant change in other cytokines and MMPs in other etiologies, considering protein concentrations or even after subdividing data according to obstructed or non-obstructed cases, suggests a high degree of variance in the patient population exists in terms of how their central nervous system and immune system responds towards recovering, compensating or aggravating hydrocephalus pathophysiology. This may be addressed by increasing the sample size to identify subsets, by standardizing and establishing a physiological grading system showcasing the stage/severity of hydrocephalus beyond clinical presentation8, 10. Additionally, in future work, it would be worthwhile to consider new classification or gradation schemes that correlate signs of physical obstruction of the shunt with the CSF quality or characteristics to eliminate out underlying subjectivity or variances.
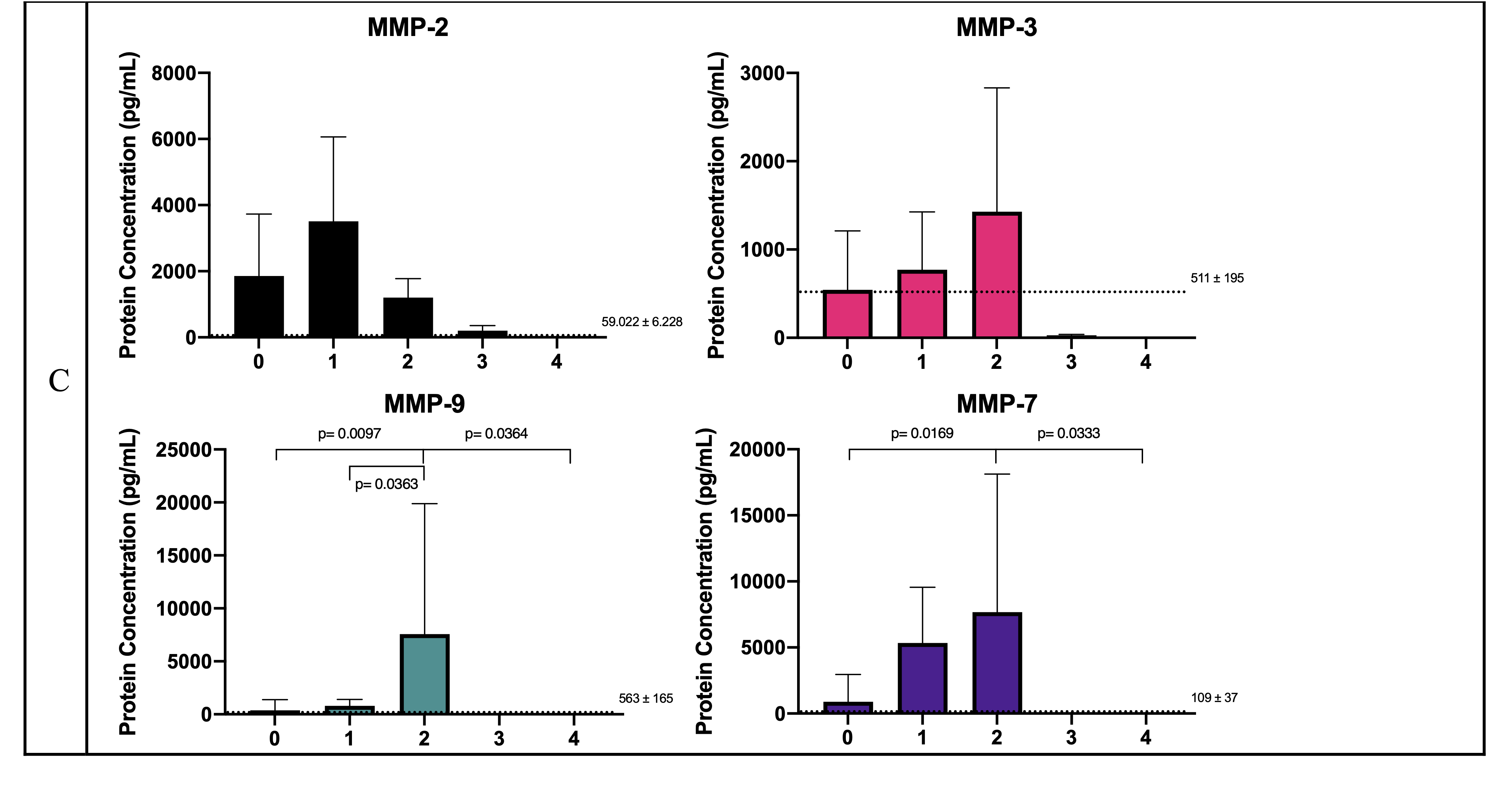
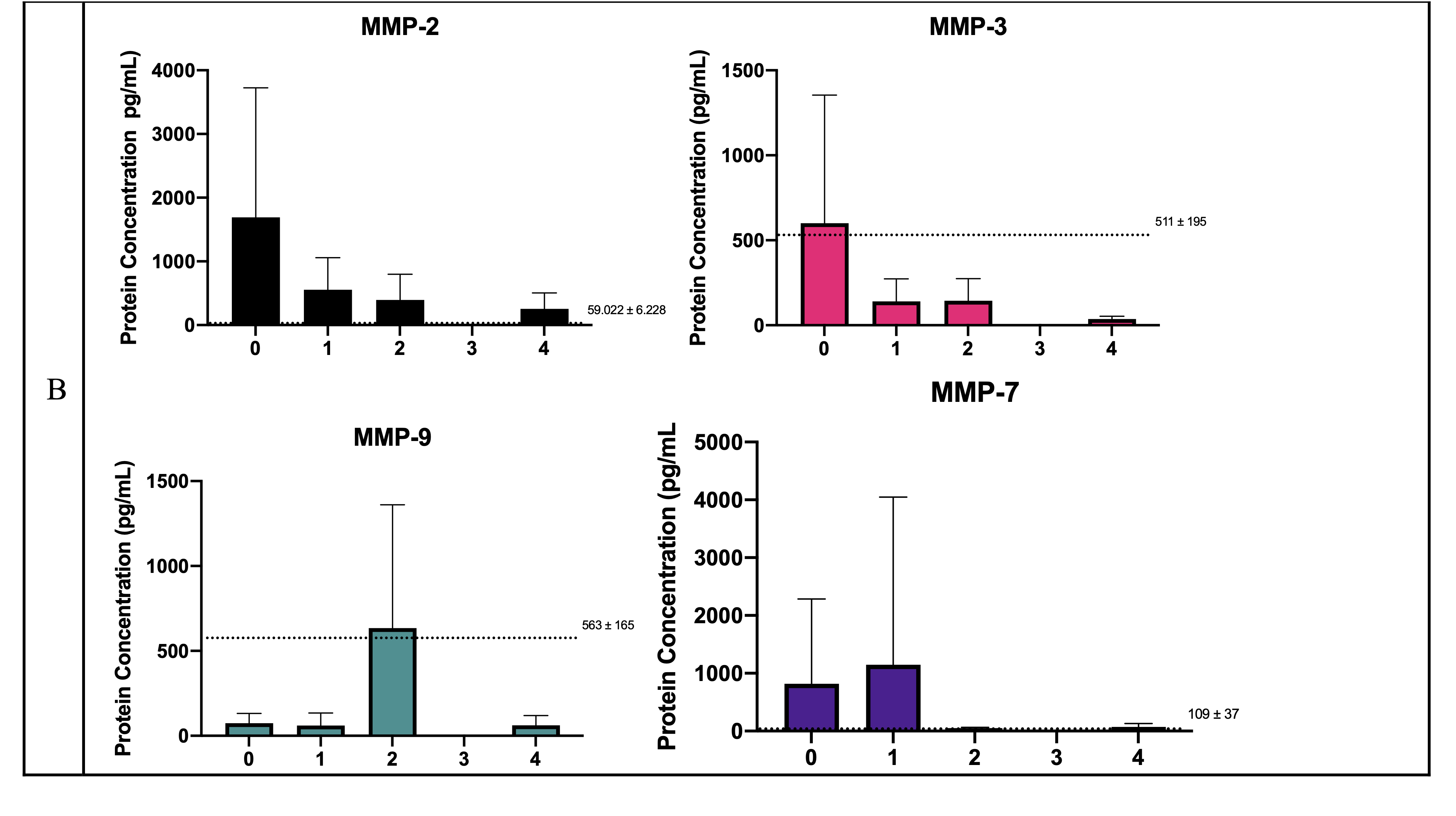
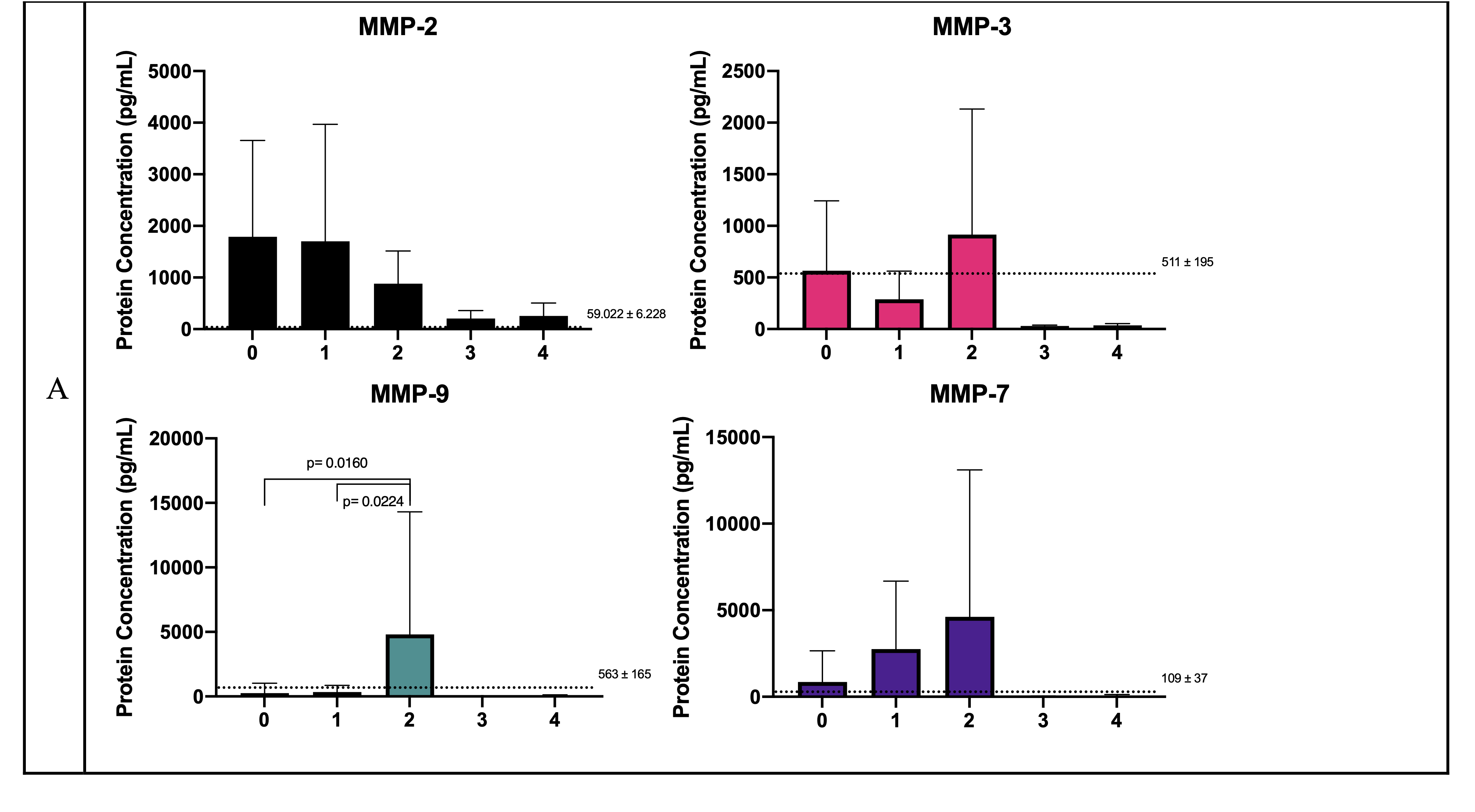
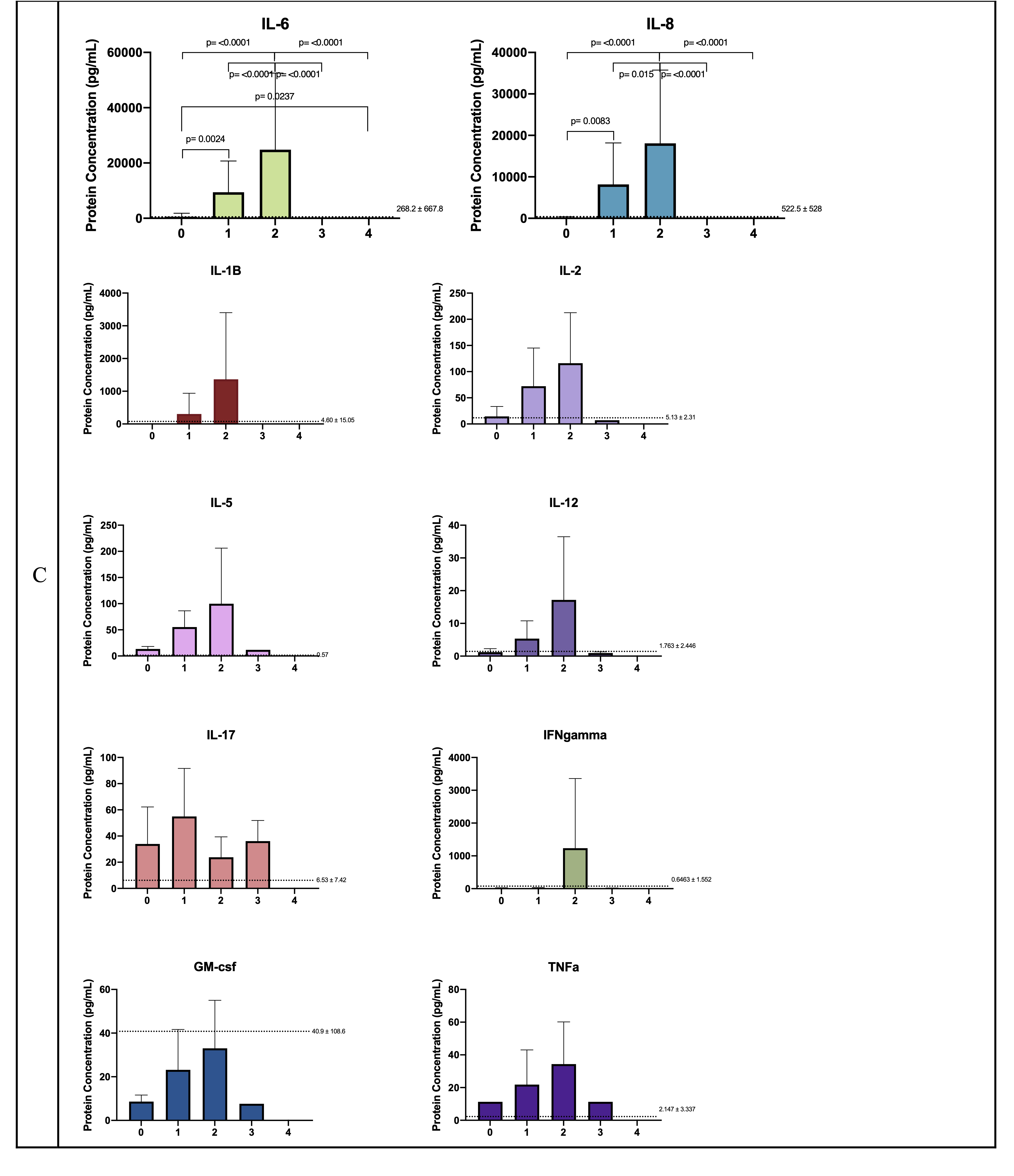
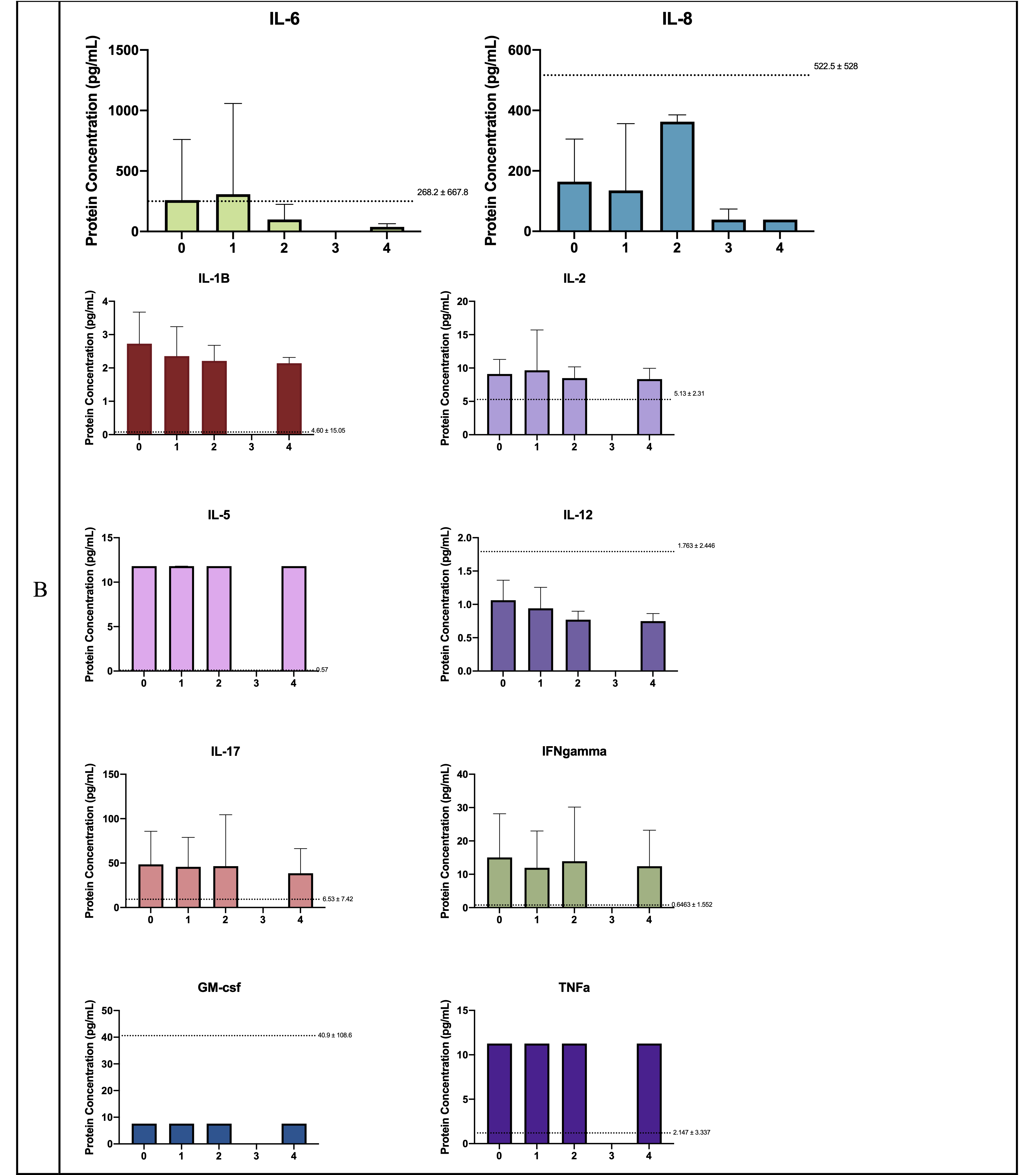
Parsing the data according to past number of revisions reveals that none of the analytes are significantly increased in obstruction cases. However, in the non-obstructed cases an interesting trend persists. protein concentration levels for IL-10, IL-6, IL-8, MMP-7 and MMP-9 significantly and progressively increase from zero to two past revisions but then sharply drop for patients coming in with three past revisions. It should be noted those patients who came in with three past revisions only had their shunts implanted for less than four days and required revision. Whereas, the seven patients who came in with four or more past revisions had theirs left implanted for more than five years and needed revision after said extended length of time due to obstruction in four of seven cases. This presentation may very well be due to the fact that patient CSF was collected at the time of shunt failure/revision surgery. Meaning, that the elusive event(s) which may be responsible for CSF shunt system failure may already have come to pass prior to or as the patient’s symptoms developed, and even decayed by the time CSF was collected. Additionally, small sample sizes per bin limit our ability to detect significant relationships in the obstruction cases as none of the cytokines significantly changed between the different revision attempts. However, as obstruction remains the most common reported reason for shunt failure, a more comprehensive, larger sampled review of CSF cytokines would aid towards understanding the mechanisms driving shunt obstruction19.
The lack of a clear neuroinflammatory response brings into question the role of neuroinflammation and CSF cytokines and MMPs as a driving force behind obstruction and consequent shunt failure. A longitudinal study with a large patient cohort and comprehensive in nature would be able to discern why protein concentration levels for major cytokines such as IL-10, IL-6 and IL-8, as well as MMP-7 and MMP-9 drop to healthy control/baseline levels by the third revision. Such a study would also answer whether revisions are still required despite the low presence of major neuroinflammatory cytokines in the patient CSF and thus, tell us of the extent of a role neuroinflammation plays in causing obstruction and/or shunt failure in HCP patients. Overall, IL-10, IL-6 and IL-8 consistently standout and may provide inspiration for therapeutic control of neuroinflammation and mitigating poor clinical outcomes such as shunt failure.
Investigations into the dependency of the length of time implanted suggests three months or less as the marked time with significantly increased concentration of IL-6, IL-8, and MMP-7. While the six months or less is identified as the most vulnerable age with significantly increased concentration of IL-6, IL-8, and MMP-7. It is intuitive that the shortest length of time has the highest protein concentration of neuroinflammatory cytokines as the risk for shunt failure is highest in the early stages of the disease and as it decreases over time and over number of revised shunts43. This indicates that the CSF cytokines evaluated in this paper, and their subsequent effects on activating immune responses in vivo, are measurable and could be useful in quantifying the degree of severity in the clinic as a useful biomarker. Thus, further arming physicians to make informed clinical decisions about their patients. It is most curious that IL-6, IL-8, and MMP-7 are significantly increased in both early implantation time and infant age groupings. As infants are arguably the most vulnerable group suffering from hydrocephalus6,9, the presence of neuroinflammation and dysregulated MMPs could be contributing to loss of tissue integrity, worsening of clinical symptoms and signs, and consequently impeding neurological development3,4. Therefore, the interplay of IL-6, IL-8, and MMP-7 and the role they play in hydrocephalus pathophysiology is worth future investigations to improve our understanding of the molecular and cellular events driving hydrocephalus.
The pro-inflammatory cytokines that stand out as elevated are IL-6 and IL-8, which is in line with previously published literature on neurologic damage in hydrocephalus29. IL-6 is a major cytokine involved in development, neurogenesis, brain injury and neurodegeneration, in addition to mounting an immune response and inducing astrogliosis, astrocyte proliferation, and angiogenesis for recovery in the central nervous system30,31. While IL-8 behaves in many similar ways as IL-6, it retains a longer half-life32–34. IL-10 is recognized to promote neuronal and glial cell survival and by inhibiting pro-inflammatory cytokine production to decrease neuroinflammation35, 36.
We show that in addition to pro- and anti-neuroinflammatory cytokines, as well as MMPs have heterogenous presentation in hydrocephalic CSF. Collectively, MMPs have been known to digest extracellular matrix proteins, but little is known about their neuroprotective or neuroinflammatory role in hydrocephalus. MMPs in the brain play a role in neurogenesis, central nervous system survival and development, neuronal myelination, integrity of the blood-brain barrier, and neuroinflammation inhibition37–40. Some studies have shown increased MMP-9 disrupts the blood-brain barrier and could even be responsible for spontaneous hydrocephalus44,45, while others have shown, in infants with PHH, MMP-9 can help them overcome symptoms of hydrocephalus46. Therefore, before claims can be made toward therapeutic directions, further investigations and characterization of MMP-7 and MMP-9 are required to understand the extent in which they influence hydrocephalus pathophysiology.
It has been purported that IL-8 and IL-10 have a dichotomy towards brain volume, as well as grey and white matter formation and that their interaction can significantly modulate neuroinflammatory responses41. In our study, with the exception of age CSF IL-8 and IL-10 protein concentrations are significantly increased in almost all of the interdependencies examined. It may be interesting to investigate if supplementing endogenous MMP-9 and IL-10 production in a time-sensitive manner can mitigate the onslaught and severity of hydrocephalus, in cases where an aggravated immune response is not warranted such as displacement, disconnection, loculation or valve disfunction.
Many questions remain about the nature and pathophysiology of hydrocephalus. Development of a suitable in vivo model of HCP to determine the degree to which glial cells are present and activated in a neuroinflammatory or neuroprotective phenotype would allow us to see if CSF IL-6 and IL-8 can serve as therapeutic targets in the hydrocephalus brain, serve as diagnostic markers for the degree of severity of hydrocephalus, or if they should be left unmitigated due to the myriad of events IL-6 and IL-8 are involved in the brain and their systemic integration in innate and adaptive immune responses26, 28. Suppression of pro-inflammatory CSF cytokines such as IL-6 and IL-8, perhaps through treatment with biologics with demonstrably efficacy to blunt subsequent immune responses, may bring reprieve to individuals suffering from hydrocephalus and lessen the blunt of their symptoms42. Additionally, future work can look towards relationships between CSF protein concentrations and patient physiology. For instance, comparisons with factors such as BMI, and lifestyle, as well as the relationship to ictus and ventricular size.
Limitations:
A likely potential side effect of CSF being collected at one center is the high occurrence of PHH in our dataset. This study also suffers from small sample size, which becomes apparent when data is parsed and grouped by obstruction or non-obstruction/other reasons for revision surgery. This study also heavily relies on the surgeon’s observations at surgery –obstruction or non-obstruction, it does not evaluate the nature of the obstruction, the degree of the obstruction nor its localization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}