The present systematic review and meta-analysis provides a comprehensive understanding of the effect of vitamin C monotherapy on sepsis in animal studies and human RCTs. The primary outcome was mortality at the longest available follow-up. The results demonstrated that vitamin C was associated with decreased mortality in both septic animals and patients with sepsis. Different secondary outcomes were reported in animal and human studies. In animal studies, the pooled data showed that vitamin C had a beneficial effect on MAP and capillary density but had no effect on the level of lactate. In human studies, the results showed that vitamin C could reduce the duration of vasopressors but could not shorten the length of ICU stay or the duration of mechanical ventilation. No adverse effects were reported, which shows the safety of intravenous vitamin C administration in clinical treatment.
Vitamin C is an essential vitamin with a variety of physiological actions, including antioxidant, the synthesis of steroids and catecholamine, regulation of the function of immune and endothelial cells, and promotion of wound healing [46]. In sepsis, vitamin C depletion dramatically increases, and its concentration decreases, which is accompanied by more severe organ dysfunction and worse prognosis. Therefore, vitamin C may be an important therapeutic option in sepsis. Animal and human studies have supported a scientific basis for vitamin C having beneficial and therapeutic effects on the host response to sepsis. Our systematic review focused on whether intravenous vitamin C monotherapy could improve prognosis, especially mortality in sepsis.
As shown in Table 2, 4 of the 7 included animal studies reported mortality, with different available follow-up times, including 24 h[39, 42], 48 h [43], and 7 days [44]. We found that the mortality of the vitamin C group was significantly lower than that of the control group. This finding is closely related to the improvement of the secondary outcomes (MAP and capillary density) by vitamin C. Our study further reviewed the mechanisms underpinning the protective effects of vitamin C supplementation in sepsis, including the prevention of microvascular dysfunction [39, 40, 42], regulation of vaso-regulatory gene expression[41], and inhibition of iNOS expression[40, 42].
Several factors influenced the quality of the animal studies. The first was the different animal species. Two animal species were used in the included studies: rats in 4 studies and mice in 3 studies. Generally, it is thought that rat models have a higher clinical relevance than mouse models [47]. Second, the type of sepsis model was different. Cecal ligation and perforation were chosen in all the studies except one, which used the method of E-coil endotoxin or cecal ligation and incision. Third, there were large variations in the time, frequency and dosage of vitamin C administration. It seems that pre-septic administration is better than post-septic administration, and large doses are better than small doses. In addition, the SYRCLE risk bias of all animal studies was high due to selection bias, performance bias, detection bias and other bias. These factors increased the heterogeneity and decreased the quality of the animal studies. Therefore, we could not obtain definitive conclusions from animal evidence.
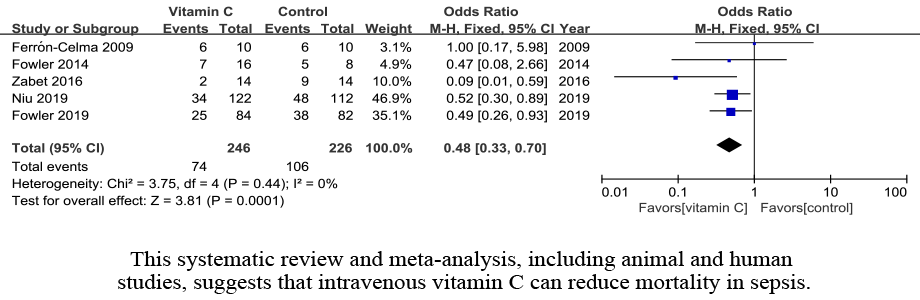
Human studies have provided more evidence for individual vitamin C strategies. Five RCTs met the standards of this meta-analysis. Among these, two recent RCTs by Fowler (CITRIS-ALI trial) and Jing-jing Niu et al. investigating the role of intravenous vitamin C in septic patients were included in this meta-analysis for the first time. The CITRIS-ALI trial reported in 2019 was a randomized, double-blind, placebo-controlled, multicenter trial with 167 patients. The Jing-jing Niu et al. study was a randomized, double-blind, placebo-controlled, single-center trial with 234 patients. The other three RCTs were all single-center trials with small sample sizes. All the trials observed 28-day mortality, except one that observed 6-day mortality [26]. The conventional analysis showed that the mortality in the vitamin C group was significantly decreased compared with that in the control group. Consistently, a previous meta-analysis, including 2 RCTs and 1 retrospective study with 146 septic patients, reported a marked reduction in mortality in the vitamin C group [31]. In contrast to our results, a meta-analysis conducted by Zhang and Jativa [48] with 5 studies (4 RCTs and 1 retrospective study) enrolling a total of 142 adults with critical illness was performed, and the result showed no difference in mortality between the control and vitamin C groups. Moreover, an updated meta-analysis [32] reevaluated the value of vitamin C treatment in patients with sepsis, and the data from 10 studies (4 RCTs and 6 retrospective studies) involving 1671 patients did not show any beneficial effect of vitamin C on mortality. We presume that this discrepancy might be explained by the following aspects. First, unlike the two previous meta-analyses, all human studies included in the present meta-analysis were RCTs, and retrospective studies were excluded. Second, the populations of our meta-analysis (patients with sepsis) and the previous one conducted by Zhang and Jativa (adults with critical illness) were different. Third, we only focused on the isolated intravenous administration of vitamin C in the treatment group, while vitamin C was prescribed along with thiamine and steroids in most of the included studies in the updated meta-analysis. The beneficial effects of vitamin C as a part of combination therapy in sepsis have been reported by previous studies, but the effect of the isolated administration of vitamin C is unclear. This meta-analysis revealed that intravenous vitamin C as a monotherapy was associated with an obvious reduction in mortality in sepsis. For the primary outcome, heterogeneity was not significant, and the GRADE assessment showed a moderate quality of evidence.
In addition, intravenous vitamin C was significantly associated with a decreased need for vasopressor support in patients with sepsis. Because vitamin C can synthetize catecholamines, exogenous supplementation increased the plasma concentrations of vitamin C to dozens of times the physiological level, which enriched endogenous catecholamines so that vascular tension and reactivity were improved, resulting in a reduction in exogenous vasoconstrictive drugs. Consistently, a series of studies reported that vitamin C might reduce the duration of vasopressor support in sepsis or septic shock [24, 49]. A recent meta-analysis of human studies revealed that intravenous vitamin C supplementation was associated with a decreased demand for vasoconstrictive drugs in critically ill patients [48]. However, it is noteworthy that vitamin C was not associated with the length of ICU stay or duration of mechanical ventilation in our systematic review. The reason might be attributed to the limited number of studies, small sample sizes and high heterogeneity. For these two outcomes, the GRADE assessment showed a low quality of evidence.
It is well known that oral and intravenous administration lead to substantially different plasma concentrations of vitamin C. The maximal saturation of vitamin C is approximately 500–1000 mg by oral administration, while intravenous vitamin C administration can achieve 70-fold higher plasma concentrations than oral administration [50]. Since the capacity of vitamin C is dose-dependent, intravenous vitamin C was used and investigated by more physicians. In this review, one study used a lower dose of intravenous vitamin C (450 mg/day), while the other four studies used higher doses ranging from 50 mg/kg/day to 200 mg/kg/day. The duration of treatment was more than 3 days. No adverse effects were reported, even in the group administered the highest dose of intravenous vitamin C. Although the optimal dose of vitamin C is unknown, an adequate dose of intravenous vitamin C for at least 3 days is needed to normalize plasma concentrations and improve outcomes in patients with sepsis.
A major strength of this meta-analysis is that we investigated the effect of intravenous vitamin C as a monotherapy on outcomes in sepsis. As opposed to studies of vitamin C in combination therapies and/or via different routes of administration, our study results can show the effect of vitamin C more clearly. Moreover, we reviewed both animal and human studies with clearly reported outcomes, which makes the results more comprehensive and compensates for the lack of human research. Additionally, all the included human studies were RCTs, and two recent RCTs with larger sample sizes had not been included in any previous meta-analyses. Findings from RCTs are considered to be more transparent and consistent. Finally, GRADE assessment was conducted in this meta-analysis to estimate the external validity of the evidence in human studies. We appraised that it is helpful for clinical decision making.
There are several limitations in this systematic review. First, the SYRCLE risk of bias summary showed that all animal studies had high bias, so the overall effects might be spurious. Second, publication bias could not be assessed due to the limited number of included studies. Third, low plasma levels of vitamin C are associated with adverse outcomes, including severity of organ failure, disease and mortality. However, we excluded populations with vitamin C deficiency and ignored the plasma levels of vitamin C in the enrolled patients. Therefore, no assessment was performed in the ascorbate-deficient population. Fourth, because only five human studies were included, the subgroup analyses of different doses to find the optimal dose of vitamin C were limited. Finally, focusing on the isolated administration of vitamin C may exaggerate its effect because some of the included patients received hydrocortisone, one recommended treatment in sepsis, especially in septic shock. However, hydrocortisone and vitamin C have several common functions, which will increase the effect of vitamin C.
{kind=link}