First, we will present the prescriber related findings of the qualitative study and the knowledge co production workshop followed by description of patient related findings of the qualitative study and the workshop.
Prescribers
A. Qualitative formative study
Participant characteristics
The sample included 20 prescribers including general practitioners (50%), family medicine practitioners (44%) and dentists (6%). Most were females (69%) and from Gezira State (82%). Prescribers’ professional experience ranged from 1-24 years (median = 5.4 years).
Factors influencing prescription of antibiotics
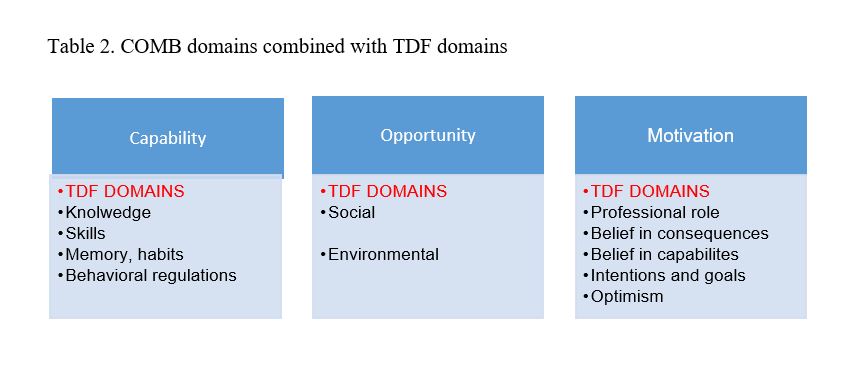
Seven TDF framework domains out of fourteen influenced the prescription practices were identified; knowledge on antibiotics and AMR, skills to answer patient demands, prescription habits and psychological reactions, social influences, intentions to change current prescription practices, belief in capabilities to change prescription practices, and environmental factors. As the study is operational, the findings of each domain are described separately to further place them in the behavior change framework.
Knowledge on antibiotics and AMR
Respondents explained that they don’t have enough knowledge or guidelines on the various classification and types of antibiotics as well as clinical indications. They believed that their knowledge was outdated. They also rarely meet representatives from pharmaceutical companies whom they considered potential sources of new information on antibiotics.
“I no longer remember which antibiotics are broad-spectrum and which are narrow spectrum. Therefore, it is not easy for me to change my practices.” (A female general practitioner) Respondents did not think that AMR was a much-discussed topic among doctors in Sudan. They explained witnessing patients with resistant infections in their practice but not knowing the actual scope of the problem globally or nationally.
“Yes, we see cases of resistant bacteria. We just change the antibiotic until it works. I don’t know if there is more resistance than before.” (A male general practitioner)
Physician skills to answer patient demands of antibiotics
Respondents felt that they lack capabilities to convince patients who demand unnecessary antibiotics. This was considered particularly challenging with patients who had predetermined the need for a specific type of antibiotic and those who had health insurance program that provides free medications. Respondents explained that patients also used emotional pressure on prescribers presenting themselves as underprivileged citizens for whom antibiotics were the only available resource.
“There are patients who have diagnosed themselves based on their symptoms, decided on the investigations and the treatment required. Not much you can do to convince them otherwise.” (A female pediatrician)
Habits and exhaustion
Treating physicians described various prescription standards and habits they developed over the years. For example, some explained prescribing antibiotics to all patients with symptoms of urinary tract infections or typhoid. Others described that they always prescribe broad spectrum antibiotics to all patients coming from long distances and to patients at risk of secondary bacterial infections.
“I have patients who walk three hours to come to the facility, so I know that they won’t be coming back for a follow-up visit. That’s when I prescribe them broad-spectrum antibiotics” (A female dentist)
Respondents highlighted that when they were exhausted from work, they just respond to the patients request and prescribe unnecessary antibiotics without discussion.
“But when you are tired, you have no energy to debate with your patient.” (A female general practitioner)
Social influences
Respondents’ social networks were often mixed with their professional networks meaning that patients were often also friends, neighbors or family members that made refusal to prescribe unnecessary antibiotics difficult.
“It is hard if I know the patients and I know his family. I am embarrassed to deny his requests. It is not easy.” (A female general practitioner)
On the other hand, some respondents also noted that respect and trust among family and friends made antibiotic negotiations with them easier.
“My family always consults with me, they trust me and I always give them my honest answer to everything. So I don’t have pressure to prescribe from that direction.” (A female general practitioner)
Intention to change prescription practices of treating physicians
Respondents explained that they had never paid attention to their antibiotic prescription practices and they don’t see any urgency to change them. They clarified that their patients would not accept alterations in their practices. Others explained that they have no intention to change their practices as they are observing an increasing number of patients with uncured infections that makes them always prescribe antibiotics that are broad spectrum.
“No, I don’t think this is what I will be doing. In general, doctors are moving to stronger antibiotics, especially if you go to private clinics you will find this.” (A male general practitioner). Prescribers also believed that reducing prescriptions of antibiotics would not eliminate the unnecessary use as patients could always buy them from community pharmacies.
“Pharmacies are always open for patients.” (A female general practitioner)
Respondents noted that patients who treat themselves with antibiotics (self-medication practices) for long time periods before visiting the health centers, made it challenging to change the type of prescribed antibiotic to narrow-spectrum.
“Many patients come to me after they had tried several antibiotics. I get very confused and wonder what antibiotics I should prescribe. Narrow spectrum is rarely possible” ( A male general practitioner)
Environmental factors
Respondents highlighted that the health insurance system which provides free treatment to patients encouraged them to demand antibiotics and perceive this as their right irrespective of the clinical indication.
“All of my patients, but especially those with health insurance, expect to get antibiotics from our center. This is the main reason they come here.” (A female general practitioner)
Prescribers explained that the availability of narrow spectrum antibiotics was rather limited in PHCC, and the availability of broad-spectrum antibiotics has increased over the years which also encourage their prescription.
B. Knowledge co-production workshop for prescriber intervention
Workshop participants reviewed the findings of the qualitative research and discussed the type of barrier each domain represented for changing the prescription practices of doctors in primary healthcare centers. This was followed by discussions about which of these domains and barriers were relevant, acceptable and practical in the context of Sudan. The selected barriers included lack of knowledge on antibiotics and AMR, lack of negotiation skills to convince patients not to take unnecessary antibiotics, and limited intention to change behavior.
Based on the BCW, the workshop participants agreed that lack of knowledge should be addressed with an educational BCT to enhance the knowledge of prescribers on the principles of antibiotic treatment and provide background on AMR. Discussions also focused on the importance of a training based BCT to improve negotiation skills to answer patient’s demand.
Workshop participants agreed that educational interventions are generally appreciated by physicians and these activities could be organized on a large scale. However, they recommended that building negotiation skills will attract fewer clinicians as it is a non-medical training. Enablement and modelling were selected as BCTs to motivate change by promoting ethical principles and by giving examples of change. Modelling was considered highly context appropriate in a hierarchical health system were senior doctors are highly respected and accordingly could be used to inspire change. The behaviour change framework for prescribers can be found in table 3.
Patients
A. Qualitative formative study
Participant characteristics
Eight FGDs were conducted with 94 patients. Most were women (73.4%) originating from Gezira State (97.9%). Participants had completed various levels of education including university (32%), preparatory school (6.3%), secondary school (36.2%), or primary school (10.6%). Some respondents had no schooling (8.6%).
Factors influencing patient behavior
Five domains of TDF related to patient demand for antibiotics were identified: antibiotic use habits, social influences, professional role of prescribers, belief in capabilities to stop demanding antibiotics, and intention to stop demanding antibiotics.
Antibiotic use habits
Respondents explained they consume antibiotics all times for any health problem or symptoms including common cold, recurrent infections such as malaria, pain, fever or fatigue. They also explained keeping antibiotics at home in case someone gets sick. This type of home pharmacy is usually filled before the holidays.
“In the community where I live, we commonly use Cipro for typhoid and everyone uses Amoclan. It works.” (A woman from El Mekky village)
Respondents explained that many people usually have preferable specific types of antibiotics that they use for all health problems and symptoms. It is usually an antibiotic that provided good results in the past. They also believe antibiotics are essential for cure; believing one could not recover from the infections without the use of antibiotics.
“People from that area commonly come to our village health unit and pharmacies to buy the same type of antibiotic. They all use the same antibiotic.” (A woman from Al Atra village)
Antibiotics were considered the fastest, strongest type of medication. Imported and more expensive antibiotics were perceived more effective than local or cheaper ones.
“I always insist on the Jordanian ones. Sudanese antibiotics are weak.” (Woman from Debagha village)
Social influences
Respondents highlighted the important role their families, friends and neighbors played in advising them on the use of antibiotics. Usually elderly females in the household were the most knowledgeable. Mothers of young children frequently chatted with one another and learned about antibiotics through experience and word by mouth. Respondents also explained that villages had knowledgeable individuals who provided advice about antibiotics.
“I can advise my neighbor on what to give to a sick child and even tell her the dosage without weighing her.” (A woman from Arkaeet village)
Professional role
Respondents frequently highlighted that many doctors prescribed the same antibiotic to all patients regardless of their health problem blaming physicians of not having enough information on antibiotics.
“Some doctors prescribe the same antibiotic over and over again … they may not know much.” (A woman from El Mekky village)
Pharmacists, on the other hand, were often seen as being able to diagnose patients and prescribe antibiotics. Respondents explained that they frequently consulted community pharmacists on antibiotic use.
“If we talk about senior pharmacists, they are comparable to medical doctors. They are called doctors too.” (A man from Al Atra village)
Belief in personal capabilities
Respondents believed in their ability to diagnose illnesses and to choose the type of antibiotic required, especially for common infections. They also believed that they knew best what works for them; not all antibiotics were believed to work for everyone.
“I know what is effective for me not the doctor. She does not know me so it is difficult for her to know what works best.” (A woman from Debagha village)
Intention to change behaviors
Respondents had no plans or goals to change their current practices of insisting on certain types of antibiotics.
“I am not planning to stop asking for antibiotics. We need them.” (A woman from Arkaweet village)
Knowledge co-production workshop for prescriber intervention
The workshop participants identified three barriers to be addressed in the behavior change strategy including habits, social influences, and intention to change behaviors (Mitchie et al 2014). They recommended to use enablement as a BCT to change habits by addressing misconceptions that patients had about antibiotics. They also recommended to use enablement by building trust between the two parties. BCTs addressing social aspects were considered highly suitable for the context of Sudan. In addition, workshop participants believed that intention to stop demanding antibiotic should be increased by providing information on consequences of such behaviors, including the spread of AMR. Workshop participants thought that patients would be eager to receive such as an educational intervention. It would be easy to implement and even to run on large scale as the network of health units is large in Sudan. the behavior change framework can be found in table 3.
{kind=link}