Studies rarely on the relationship between elevated Lp (a) and the occurances of MACE in patients with ACS,despite the increasing number of ACS patients. Our study supported that elevated LP (a) was a useful marker for predicting adverse prognosis after coronary angiography in Chinese patients with ACS. And what's more, patients with simultaneous increases in LP (a) and TSH exerted the highest risk, suggesting that such patients may need more aggressive Lipid lowering program.
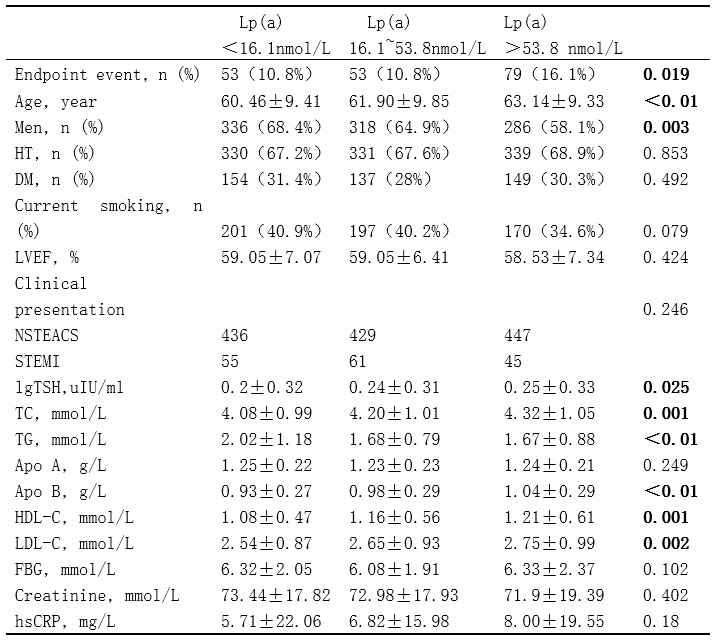
It had been well confirmed about the role of Lp(a) in the occurrence and development of coronary heart disease. Erqou et al. recently conducted a large meta-analysis of 36 prospective studies involving 126634 people, which confirmed the modest but strong risk of cardiovascular disease caused by elevated LP (a), especially when LP (a) ≥ 240mgl. [18]A recent study of Chinese patients with newly diagnosed coronary heart disease conducted by sun Di et al. confirmed that LP (a) was a serviceable marker for predicting the presence and severity of coronary heart disease, they found that the highest tertile of Lp(a) [Lp(a) ≥ 205.7 mg/L] significantly and independently increased the risk of coronary heart disease by 1.44 times compared with the lowest tertile. [19] However, the study about the predictive value of elevated LP (a) in patients with ACS was divergent,whatever domestic or abroad. Among 569 patients who underwent PCI and had well controlled LDL-C levels (< 100 mg / dl), patients with elevated LP (a) were more easily to be exposed to MACE events, and elevated LP (a) are independent predictors of death and recurrence in ACS patients [20]. In a similar age study, Ikenaga et al. found that elevated LP (a) in patients with AMI were associated with a higher incidence of MACE after treated with primary PCI, [21] Consistent with these findings, in our study, multivariate Cox Proportional Hazard Model revealed that LP(a) was an independent risk factor for adverse prognosis after coronary angiography in ACS patients (OR: 1.003;95%CI:1.002 ~ 1.005; P<0.01), The highest tertile of Lp(a) [Lp(a) ≥ 53.8nmol/L] increased the risk ACS by 1.704 fold compared to the lowest tertile significantly and independently. ROC analysis showed that when the cut-off value of Lp(a) was 53.6nmol/L, the area under the curve (AUC) of LP(a) in predicting MACE in ACS patients was 0.551 (95% CI: 0.505–0.597, P < 0.05), the diagnostic sensitivity was 43.2%, the specificity sensitivity was 67.6%, especially when TSH is combine. However the association between elevated LP (a) and adverse cardiovascular outcomes in patients with ACS has not been confirmed in some studies. A recent dal-Outcome trial of ACS patients treated with statins showed that LP (a) concentration was not associated with MACEAs. [20] In addition, zewinger et al., who enrolled 3313 patients with confirmed CAD and followed them for a median of 9.9 years, found no association between Lp (a) concentrations and gene variants and mortality [22].
The virgation between these studies may be due to the different sample sizes, the use of different definitions of blood lipid profile according to age, and the effects of races and nationalities on blood lipid. Previous studies have shown that the plasma TSH level increases slightly with age. [23] Therefore, it is worth discussing whether the equivocal predictive effect of LP(a) in ACS patients is related to the difference of TSH level.
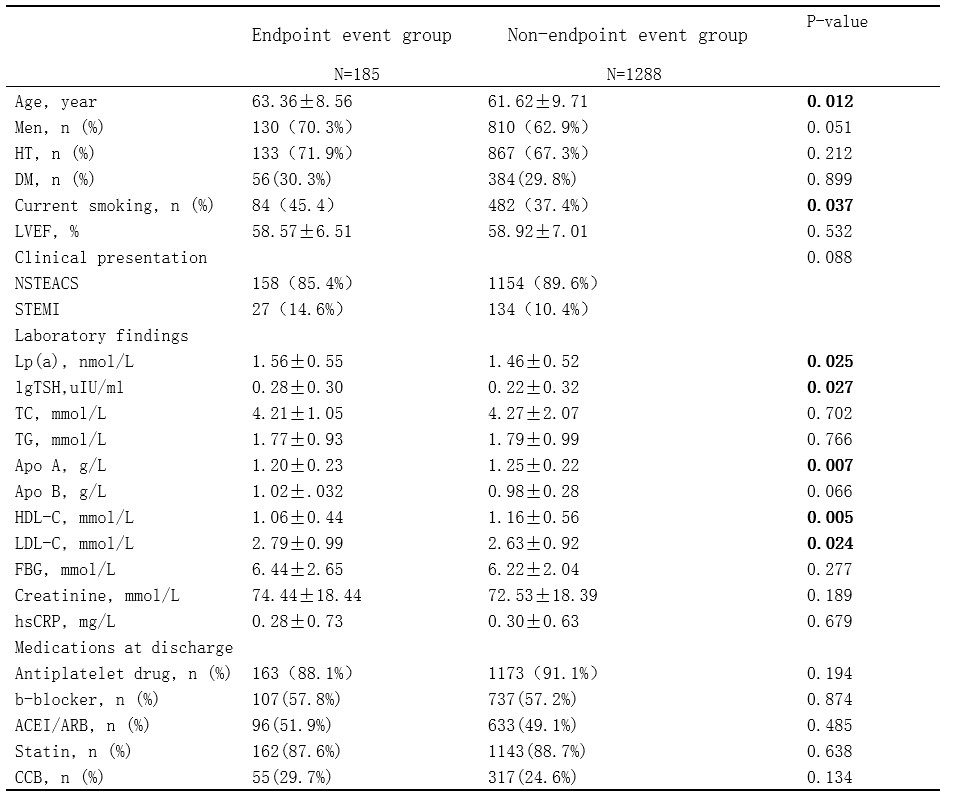
LP(a), an 18 mm diameter lipoprotein molecule bound by ApoB-100 and ApoA in which is produced of hepatic origin, whose level were regulated by a region on chromosome 6 near PLG (plasminogen gene), is markedly increased when the gene is expressed actively [24]. It was indistinct about the predictive mechanism of LP (a) in patients with coronary heart disease, a potential explanation may be that LP (a) mediates pro-inflammatory and anti-fibrinolytic effects [25], leading to atherosclerosis by interfering with lipid metabolism and fibrinolytic system. Oxidized LP (a) can promote macrophages to transform into foam cells, thereby promoting the formation of inflammatory plaques and affecting it's stability. Another explanation was that endothelial and anticoagulant functions were damaged by elevated LP (a) in promoting dysfunction of endothelial and increasing phospholipid oxidation.[26, 27] In our study, patients with elevated LP (a) levels were older, had a higher proportion of women, and had higher LDL cholesterol levels. As we all know, All these three conditions are risk factors for adverse cardiovascular outcomes. In addition, elevated LP (a) levels were also associated with increased burden of atherosclerosis and phenotype of vulnerable plaque in patients with ACS. [28, 29] And then, elevated LP (a) levels were associated with the severity of CAD assessed by GS. [19] All these provide a theoretical basis for the study of LP (a) . In treatment, PCSK9 inhibitor and ApoA antisense oligonucleotides can reduce LP (a) level, [26], but the clinical benefit of reducing LP (a) has not been determined. It is necessary to evaluate whether lowering LP (a) level can provide cardiovascular benefits for patients with coronary heart disease In future studies.
The incidence of coronary heart disease is higher in patients with the coexistence of dyslipidemia and hypothyroidism. Hypertriglyceridemia caused by hypothyroidism develops as a result of impaired removal of endogenous TG, and increased of Liver derived f triglycerides [30],it should be noted that there is also a higher TG-enriched lipoprotein(RLPs) levels in the serum of patients with hypothyroidism, which may be caused by the decrease of lipoprotein lipolysis due to the decrease of enzyme activity, or the increase of intestinal and liver production [30], and previous studies have shown that TSH levels may be positively associated with adverse lipid levels [17], however, the mechanism underlying the higher risk of adverse lipids and hypothyroidism caused by TSH is not very clear. We investigated the contribution of high levels of LP (a) and TSH to the poor prognosis of ACS patients and found their synergy to be at highest risk. Based on our observations, the predictive value of LP(a) for the outcome of ACS patients is influenced by multiple factors, such as age, gender, previous severe complications, etc., whereas plasma TSH level is perhaps the next factor of concern.
The European Society of Cardiology/European Atherosclerotic Society guidelines recommend measuring Lp(a) in patients with premature CAD. [3] European guidelines recommend a desirable level for Lp(a) as 80th percentile (less than ~ 50 mg/dL) [3], whereas it is usually 30 mg/dL for Chinese population considering the far lower level in Chinese. [31, 32] There for we suggested that a lower critical value should be used in Chinese patients with coronary heart disease.
However, there are still some limitations in this study. First of all, this study is a single center study. Second, we did not evaluate LP (a) subtype, so we could not evaluate whether there were some distinctions in the incidence of MACE after coronary angiography in ACS patients with different subtypes of LP (a). Third, the impact of elevated Lp (a) levels on clinical outcomes in ACS patients and non-ACS patients is different [16]. However, due to the lack of data, we can not make subgroup analysis by CAD subtype.
{kind=link}
{kind=link}
{kind=link}