Background information
PCOS is a syndrome complex consisting of hormonal and metabolic disturbances and their associated clinical manifestations. The hallmark of hormonal imbalance is hyperandrogenism manifesting biochemically as an elevation of testosterone (T) and increased free androgen index (FAI), with the latter reflecting an increase in the T:SHBG ratio (20). Nearly 40%-70% of women with hyperandrogenism also exhibit an elevation of dehydroepiandrosterone sulphate (DHEAS) levels (21). The metabolic manifestations associated with PCOS include obesity, dysglycaemia, dyslipidaemia, sleep apnoea, and hypertension and are exhibited by nearly 33% of women (22). The biochemical hallmark of metabolic disturbances in PCOS is insulin resistance assessed with indices such as the homeostatic model assessment (HOMA) and quantitative insulin sensitivity check index (QUICKI), which have reasonable correlations among each other as well as with insulin clamp techniques (23).
Metabolic disturbances in PCOS are accompanied by heightened endothelial inflammation, leading to an increased risk of future CV events (24). According to a nationwide survey in Denmark, the hazard ratio for CVD was 1.7 in patients with PCOS, with obesity, dysglycaemia, hypertension, and dyslipidaemia being the principal contributors (25).
The traditional management strategies for PCOS predominantly target menstrual irregularities, hirsutism, and ovulation dysfunction. The only therapeutic strategy stressed from the metabolic perspective is weight reduction by lifestyle intervention. However, with the impressive results of GLP1-RAs and SGLT-2is on both the metabolic front and the associated CV outcomes, these molecules have come into focus in the management of a broad range of metabolic disorders, such as non-alcoholic fatty liver disease, sleep apnoea, and PCOS (26-28).
Our finding
This meta-analysis was conducted to highlight the impact of SGLT-2is on metabolic and hormonal aspects of PCOS. To our knowledge, this is the first meta-analysis exploring these benefits. Significant improvements were observed in metabolic parameters, as demonstrated by reductions in body weight (SMD: -0.68, 95% CI -1.16 to -0.19, P<0.01) and FPG from baseline (SMD: -0.59, 95% CI -0.99 to -0.19, P<0.01) and improvement in the HOMA-IR (SMD: -0.39, 95% CI -0.76 to -0.03, P=0.03) with the use of SGLT-2is. No benefit on the HOMA-IR was found when the subgroup analysis was performed by excluding the placebo-controlled trial (14). One of the reasons for this finding could be the inclusion of active comparators such as metformin in the study by Javed et al. (13) and exenatide QW in the study by Elkind-Hirsch et al. (15), which could induce significant improvement in the HOMA-IR. Hence, it is highly plausible that the impact of SGLT-2is on the HOMA-IR was preserved in the subset of patients with PCOS, which is explained by their noninferiority to either metformin or exenatide QW. Regarding hormonal parameters, except for the impact on DHEAS (SMD: -0.55, 95% CI -0.94 to -0.16, P<0.01), which persisted even after the subgroup analysis, there was no significant difference observed for FAI, TT, and SHBG. The hyperinsulinaemia-induced elevation in dehydroepiandrosterone sulfate (DHEAS) could be an indicator of the risk of developing type 2 diabetes (T2D) in the future (29). A reduction in DHEAS levels, especially with increasing age, has been found to be protective against CV events (30). Moreover, the reduction in DHEAS shown here provides an interesting hypothesis wherein SGLT-2is, by their unique ability to reduce body weight and improve glucose uptake, would reduce hyperinsulinaemia, along with a reduced amount of DHEAS causing a reduction of free testosterone, which in turn would improve glucose utilization, forming a basis for breaking down the vicious cycle of hyperinsulinaemia and hyperandrogenism, the very basis of PCOS (Figure 4).
Limitations and strengths
All the studies were limited by small sample sizes, and each study investigated varying endpoints. Hence, the tested hypothesis needs to be analysed in a larger population of patients with a uniform and well-defined outcome criterion. Individual patient-related data were not available for analysis. We could not assess the extended metabolic parameters of interest, such as dyslipidaemia since data were either not presented or inadequately analysed in the studies. Finally, significant differences in the comparator arm could have skewed the data against the hypothesis.
Because of the very small number of patients recruited in the individual studies, as well as the urgent need to address the important aspect of metabolic management in PCOS, this meta-analysis is timely and pools an adequate number of patients to generate a robust hypothesis for future trials. None of the parameters exhibited significant heterogeneity, and hence, the effect size estimation was robust. The subgroup analysis was also supportive of the primary hypothesis.
Literature review
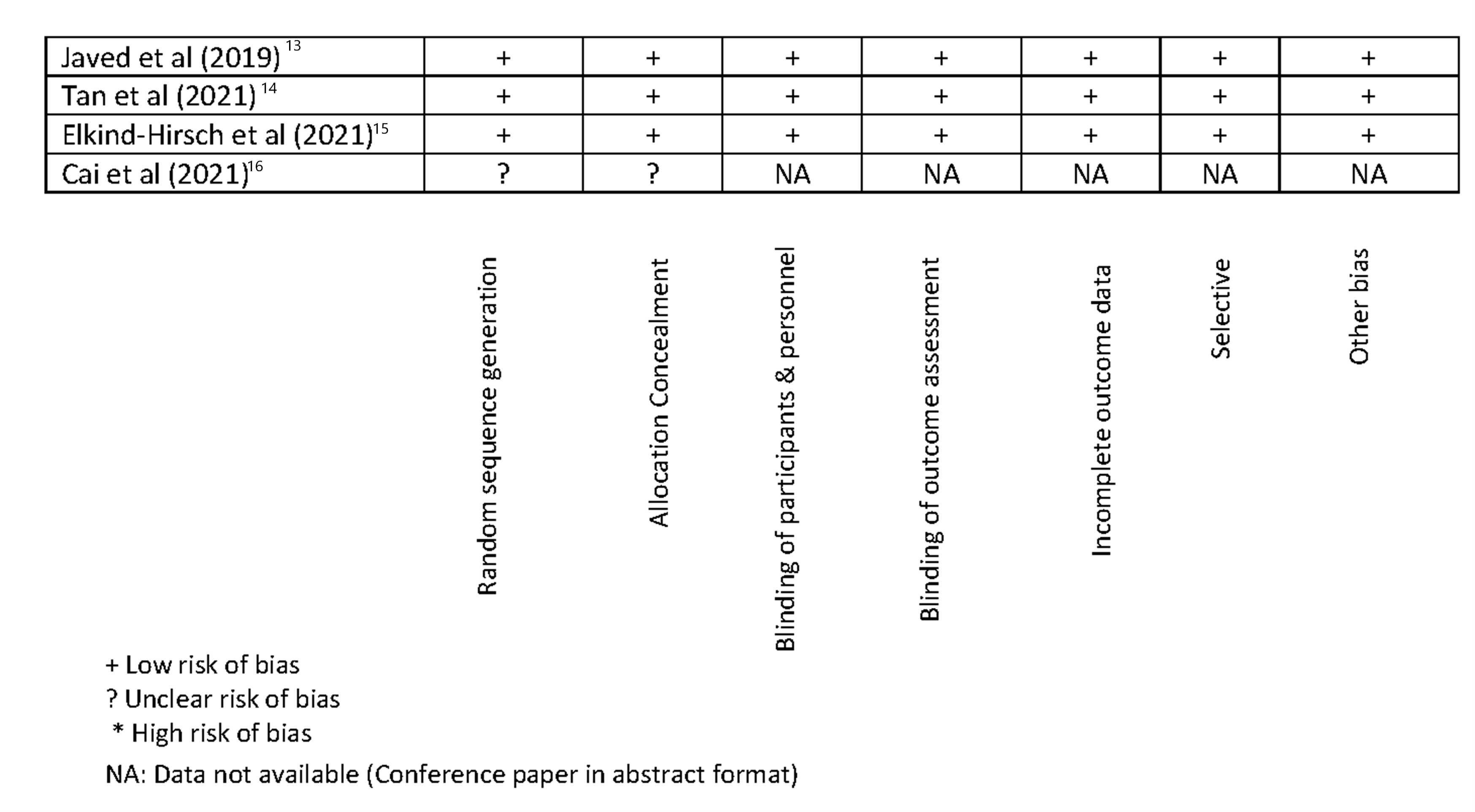
Empagliflozin was studied in 19 women with PCOS with metformin as a comparator and was found to improve body weight, basal metabolic rate, and parameters of glycaemia with a nonsignificant effect on androgens and other hormones (13). Dapagliflozin (DAPA) was studied alone and in combination with exenatide (EQW) and GLP1-RAs compared with a combination of phentermine/topiramate (PHEN/TPM). EQW/DAPA and PHEN/TPM resulted in the greatest loss of weight and total body fat according to DXA and WC. Despite equivalent reductions in BMI and WC with PHEN/TPM, only EQW/DAPA and EQW resulted in significant improvements in the mean blood glucose and insulin sensitivity (15). Reductions in fasting glucose, testosterone, FAI, and BP were observed with all drugs. In a randomized controlled trial of 53 patients in China, canagliflozin was found to be noninferior to metformin for all anthropometric, metabolic, and hormonal parameters (16). In another RCT, licogliflozin produced an improvement in metabolic parameters (14). In addition, licogliflozin usage was associated with a reduction in androstenedione and DHEAS, both precursors of testosterone, the driving force of hyperandrogenism in PCOS.
Implications for research and practice
A definite need exists for treatment options to manage PCOS, a condition with far-reaching implications in both the short term and long term, caused by a deadly nexus of metabolic and hormonal defects. SGLT-2is, by their unique mode of action, powerful efficacy, and proven cardiovascular benefits, are naturally apt candidates (26). This meta-analysis indicates the benefits of using SGLT-2is for the treatment of PCOS and provides ample evidence to look forward to the publication of large-scale RCTs currently in progress (31).
{kind=link}
{kind=link}