Patient and Setting
We prospectively enrolled all critically ill cirrhotics (CIC) who were admitted to the liver intensive care unit (LICU) of the Institute of Liver and Biliary Sciences, New Delhi from March 2017 to June 2017. The inclusion criteria were as follows: CIC of any etiology, requiring intensive care for more than 24 hours; and age ≥ 18 years. Moribund patients and those with hepatocellular carcinoma or other malignancies were excluded.
Study Plan: Baseline and daily follow-up information including the demographic, clinical, hemodynamic, biochemical, and nutritional details were collected prospectively on a structured proforma, till the patient’s stay in the ICU. All patients were managed as per the standard nutrition protocol of the institute irrespective of the nutritional status. The data was entered in excel sheet and statistically analyzed.
Diagnosis of disease: Cirrhosis was diagnosed on the basis of standard, clinical, biochemical, histological and/or radiological criteria.7
Assessment of disease severity: Child-Turcotte-Pugh (CTP) and Model for End-stage Liver Disease (MELD) scores were used to describe the severity of liver disease while Sequential Organ Failure Assessment Score (SOFA) and Acute Physiology and Chronic Health Evaluation (APACHE) scores were used to assess the severity of critical illness.
Nutritional Assessment:
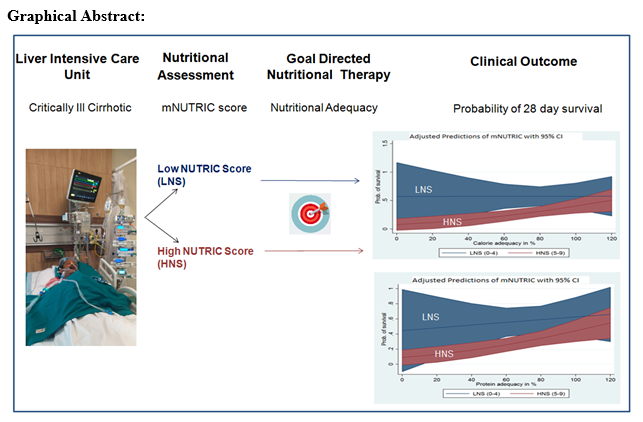
Nutritional status was assessed at ICU admission using mNUTRIC score with the point system as developed previously,8 with variables like age, number of days from hospital to ICU admission, number of co-morbidities, APACHE II score and SOFA score as shown in Table 1. Patients with mNUTRIC score ranging from 0 to 4 were classified as low mNUTRIC score (LNS) implying to be at low nutritional risk and those with a score between 5 to 9 as high mNUTRIC score (HNS), suggesting a higher nutritional risk.
Nutritional Management:
Enteral nutrition (EN) using a fine bore nasogastric (NG) tube was initiated within 24 hours of ICU admission in all mechanically ventilated (MV) patients unless patient was a bleeder, hemodynamically unstable, or had paralytic ileus. Naso- jejunal feeding was initiated only in case of feed intolerance with a failed trial of prokinectics. Non-intubated patients were given oral diet. Total Parenteral Nutrition was used only for patients with a non-functional gut. Nutritional requirements were calculated as per the standard guidelines of 35-40 kcal and 1.2-1.5 gm protein per kg ideal body weight9. Protein intake was increased up to 1.8-2 gm in case of obese patients and those requiring renal replacement therapy (RRT).
Nutritional Adequacy:
Nutritional adequacy was defined as the percentage of calories and protein actually received over 24 hours of the total energy or protein prescribed. Daily nutritional adequacy was calculated and averaged out for the total duration of ICU stay.6
Medical Management:
Patients were managed as per standard guidelines including endotracheal intubation for those in respiratory failure, coma or acute respiratory distress syndrome. Fluid resuscitation in combination with vasoactive drugs were used as appropriate. RRT was used in patients with acute kidney injury (AKI), severe metabolic acidosis, hyperkalemia and fluid overload. All the patients were screened for infection and treated empirically with broad spectrum antibiotic combinations as per the physician.
Objective:
The primary objective was to study the association of nutritional status at ICU admission with 28 day mortality. The secondary objectives were (a) to assess the effect of nutritional adequacy on the relationship between baseline nutritional status and 28 day survival probability, (b) to study the effect of baseline nutritional status on outcome parameters like duration of mechanical ventilation (MV), new onset of infections (NOI), and length of ICU stay (LOS).
Data Collection:
Apart from routine baseline demographics, information was collected on the, duration in hospital prior to ICU admission; presence of co-morbidities; decompensation status like ascites, jaundice, upper gastrointestinal bleed; presence of sepsis; reason of ICU admission including altered sensorium, upper GI bleed, respiratory distress or metabolic acidosis; disease severity scores like SOFA, APACHE II, CTP and MELD. Follow up data collected daily until the death or discharge of the patients included the hemodynamic parameters like heart rate, mean arterial pressure, requirement of vasopressors; biochemical parameters like complete blood count, liver function test, kidney function test, coagulation factors, random blood sugars; blood gas parameters like pH, PaO2, FiO2; requirement of RRT, days of MV, development of new onset infection (NOI), duration of ICU stay and the nutritional adequacy.
Definition of terms:
Sepsis: Presence of any one of the following:-pneumonia, spontaneous bacterial empyema (SBE), spontaneous bacterial peritonitis (SPB), positive minibal or blood culture and others (cellulitis, urinary tract infection, cholangitis).10
New onset of infection: Absence of infection at ICU admission but development of new onset pneumonia/ positive blood or minibal culture reports/ line sepsis/septic shock during the entire ICU stay.11
Acute kidney injury: Presence of any one -increase in serum creatinine by 0.3 mg/dl within 48 hours or increase in serum creatinine to 1.5 times from baseline or urine volume <0.5 ml/kg/h for 6 hours.12
Renal Replacement Therapy: If patient on sustained low-efficiency dialysis (SLED) or continuous renal replacement therapy (CRRT).12
Mechanical ventilator days: Total number of days on mechanical ventilation.
Length of ICU stay: Total duration of stay in ICU until death or discharge.
Statistical Analysis
The collected data was analyzed using SPSS version 22. Data are presented as mean (±standard deviation), median (range) or number (%) as appropriate. All variables were checked for normal distribution, non-normal data were analyzed using non-parametric tests. Baseline characteristics were compared between HNS and LNS groups using Chi-square test for categorical variables and Student’s t-test or Wilcoxon ranksum test for continuous variables. Logistic regression analysis was carried out to find the effect of mNUTRIC score on 28-day mortality adjusting for factors significantly different between the HNS and LNS group. P <0.05 was considered statistically significant.
{kind=link}