Study Design and Participants
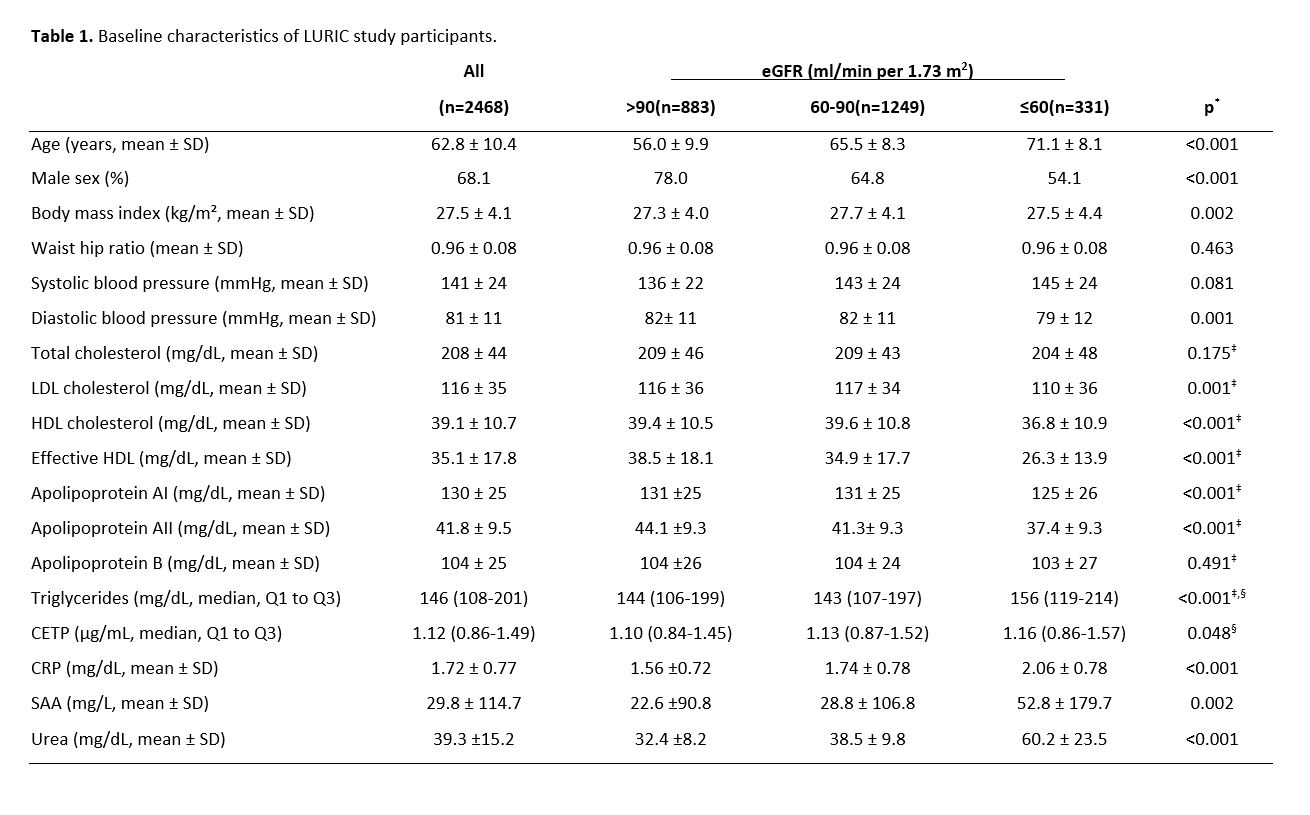
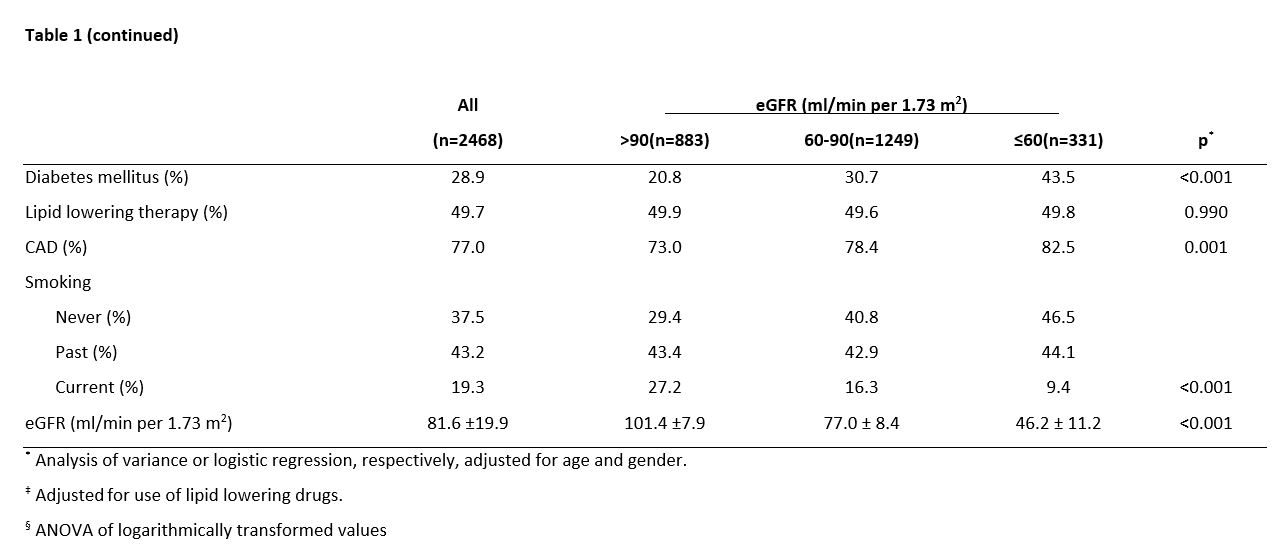
We studied 2468 participants of the LUdwigshafen RIsk and Cardiovascular Health (LURIC) study.[15] 1032 patients (29 %) of the original study population were not included in this study as not enough sample volume of serum required for cholesterol efflux measurement had been available from these patients. Inclusion criteria were: German ancestry, clinical stability except for acute coronary syndromes, and the availability of a coronary angiogram. The indications for angiography in individuals in clinically stable condition were chest pain and/or noninvasive test results consistent with myocardial ischemia. Individuals suffering from acute illness other than acute coronary syndromes, chronic non-cardiac diseases, or malignancy within the past 5 years and subjects unable to understand the purpose of the study were excluded. The study was approved by the Ethics Committee at the “Aerztekammer Rheinland-Pfalz” and was performed conform to the declaration of Helsinki (837.255.97 [1394], approved January 8th, 1999). Informed written consent was obtained from all participants. Coronary artery disease (CAD) was assessed by angiography with maximum luminal narrowing estimated by visual analysis. Clinically relevant CAD was defined as the occurrence of ≥ 1 stenosis of ≥20% in ≥ 1 of 15 coronary segments. Individuals with stenoses < 20% were considered as not having CAD. Diabetes mellitus was diagnosed when plasma glucose was > 1.25 g/L in the fasting state or > 2.00 g/L 2 h after an oral glucose load,[16] or when antidiabetic medical treatment was prescribed. Hypertension was diagnosed when the systolic and/or diastolic blood pressure exceeded 140 and/or 90 mm Hg, respectively, or when a patient was on antihypertensive medication. Information on vital status was obtained from local registries. Among the 2468 persons studied, 717 deaths (29.0 %) occurred during a median follow-up of 9.9 (8.5–10.7) years. Cardiovascular death included sudden death, fatal myocardial infarction, death due to congestive heart failure, death immediately after intervention to treat CAD, fatal stroke, and other causes of death due to CAD.
Cholesterol efflux capacity
Cholesterol efflux capacity was quantified in blood samples as described.[19] Briefly, J774 cells, derived from a murine macrophage cell line, were plated and radiolabeled with 2 µCi of 3H-cholesterol per milliliter. Cells were incubated with 0.3 mM cAMP (C3912, Sigma-Aldrich) to upregulate ABCA1. Subsequently, efflux medium containing 2.8% apolipoprotein B–depleted serum was added for 4 hours. All steps were performed in the presence of 2 µg per milliliter acyl–coenzyme A:cholesterol acyltransferase inhibitor (Sc-215839A, Santa-Cruz Biotechnology). Liquid scintillation counting was used to quantify the efflux of radioactive cholesterol from the cells. Percent efflux was calculated by the following formula: [(microcuries of 3H-cholesterol in medium containing 2.8% apolipoprotein B–depleted serum – microcuries of 3H-cholesterol in serum-free medium) / microcuries of 3H-cholesterol in cells extracted before the efflux step] × 100. To correct for inter-assay variation across plates, a pooled serum control was included on each plate. Values for serum samples from patients are given in percentage of this control (% C). All assays were performed in triplicate.
Statistical Analysis
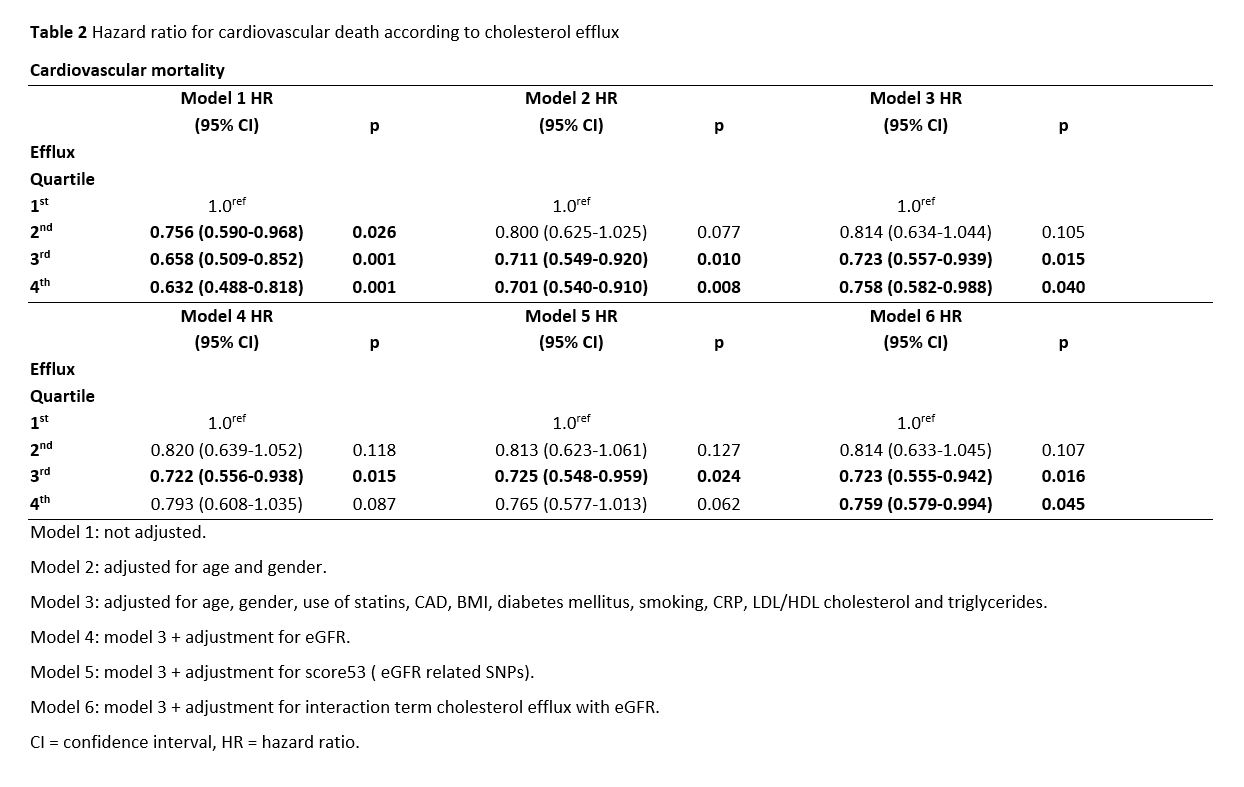
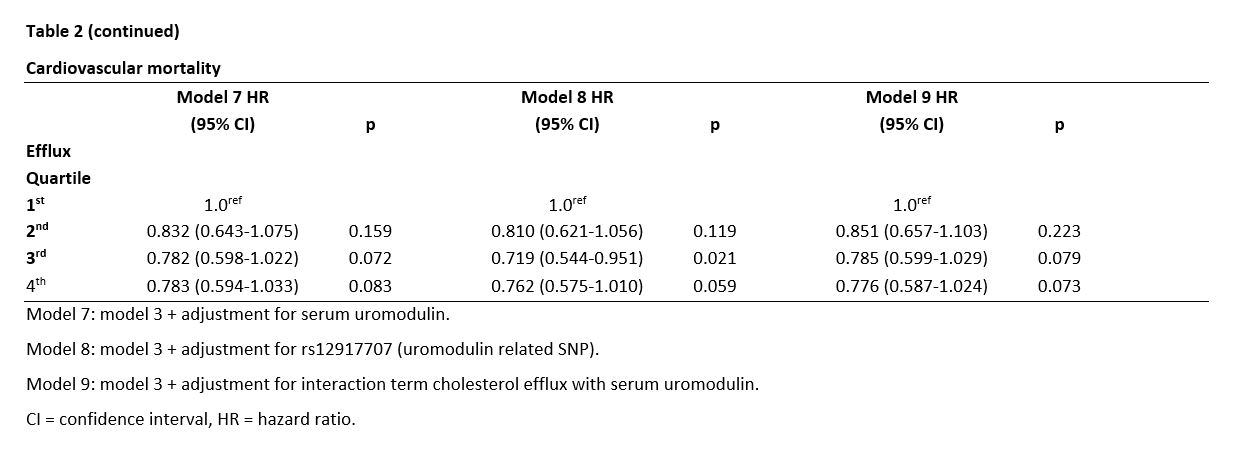
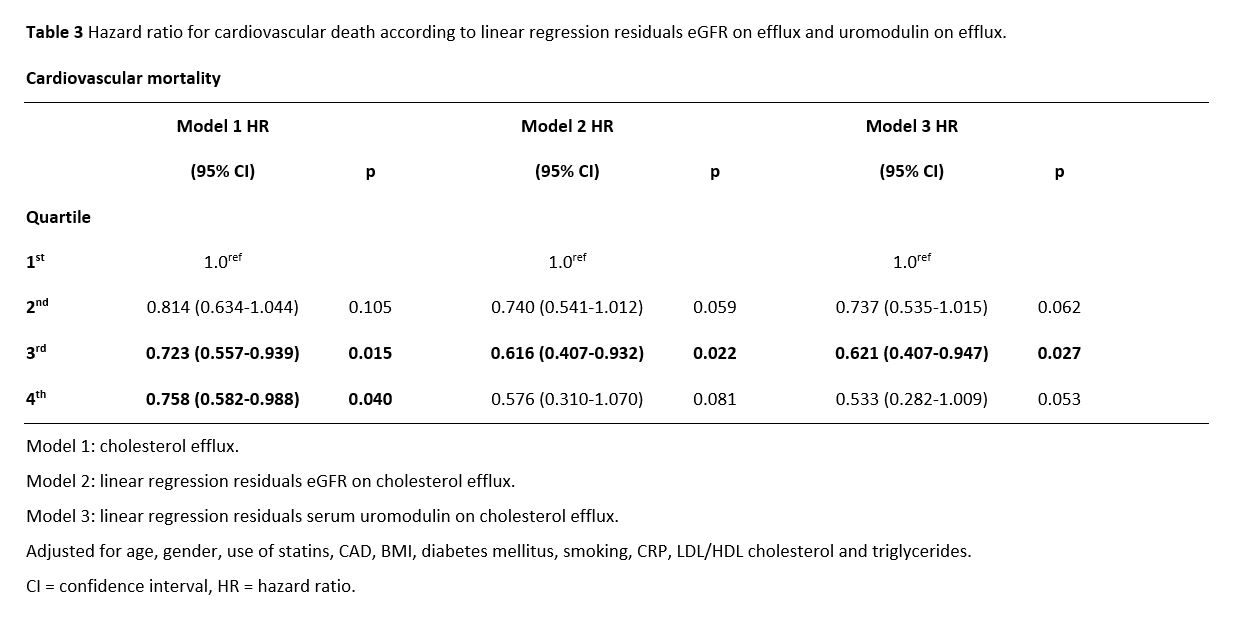
Normally distributed data are presented as mean ± SD. CETP, triglycerides, adiponectin, interleukin-6 (IL-6), and C-reactive protein (CRP) exhibited a skewed distribution and are presented as median and interquartile (Q1, Q3) range. Parameters not normally distributed were transformed logarithmically for statistical analyses. The χ2 test and Analysis of Variance were used to compare the distributions of the variables across the eGFR categories. The effects of cardiovascular risk factors, CAD-status and intake of lipid-lowering drugs on cholesterol efflux levels were determined using general linear models using cholesterol efflux as the dependent variable and age, lipid lowering therapy, CAD-status, body mass index (BMI), diabetes mellitus, smoking history (never, former, current), LDL-C/HDL-C ratio, and triglycerides as independent variables. Multivariate adjustments were performed for age, gender, intake of statins, CAD-status [none, stable CAD, unstable CAD, non-ST-elevation myocardial infarction (NSTEMI) or ST-elevation myocardial infarction (STEMI)], BMI, smoking status, LDL-C/HDL-C ratio, triglycerides, and metabolic syndrome / type 2 diabetes mellitus. A genetic score was calculated based on 53 independent SNPs related to eGFR. The effects of eGFR and cholesterol efflux capacity on the SNP-score corresponding to the sum of eGFR increasing alleles were determined using general linear models using the SNP-score as the dependent variable and age, gender, lipid lowering therapy, CAD-status, body mass index (BMI), diabetes mellitus, smoking history (never, former, current), hypertension, LDL-C/HDL-C ratio, apolipoprotein AI and triglycerides as independent variables. Cox proportional hazard models were used to examine the effect of cholesterol efflux capacity on mortality. Multivariable adjustment was performed for intake of lipid lowering drugs, age, gender, CAD, BMI, diabetes mellitus, smoking, LDL-C/HDL-C ratio and triglycerides. Moreover, the interaction term between cholesterol efflux and eGFR as well as uromodulin with regard to cardiovascular mortality was studied including the respective interaction terms as covariates. Additionally, residuals from linear regression models of eGFR as well as uromodulin on cholesterol efflux capacity were used instead of efflux capacity in the Cox proportional hazard models to test for a possible interplay between parameters of kidney function and cholesterol efflux capacity. All statistical tests were 2-sided; P < 0.05 was considered significant. The SPSS 22.0 statistical package (SPSS Inc.) was used.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}