PCNL for renal calculi was first described by Fernstrom and Johansson in 1976 [1]. The complications of PCNL include fever, infection, bleeding necessitating transfusion, and bleeding for super-selective angioembolization (SAE).
In this retrospective study, we studied and reported 665 patients receiving PCNL in our center from 2016 to 2019. The risk of hemorrhagic complications requiring blood transfusion is associated with low preoperative hemoglobin levels, preoperative infection and history of open surgery of treated kidney. The OR value found was 9.3, 15.6, 3.2 respectively.
Yamaguchi [5] and Christian [6] found that a larger tract size will increase the risk of hemorrhage during PCNL. The transfusion rate varied from of 1.1–12% when the tract size turned from 18F to 30F. In our study, we used a 20F sheath and 18F nephroscope to remove the calculi. It was defined as a medium size of sheath [5]. The transfusion rate in our study was 3.5%. In another three studies include more than 500 cases [7–9], the authors used the fixed tract size, 30F, 30F, 26-30F, respectively, and the transfusion rate was 10.8%, 0.8%, 12.3%, thus bleeding may have increased rate with the surgery performed at different centers than the size of the tract. Here we look back into six studies (Table 5) [5, 7, 8, 9, 10, 11] which include more than 500 cases and analyze our data with them.
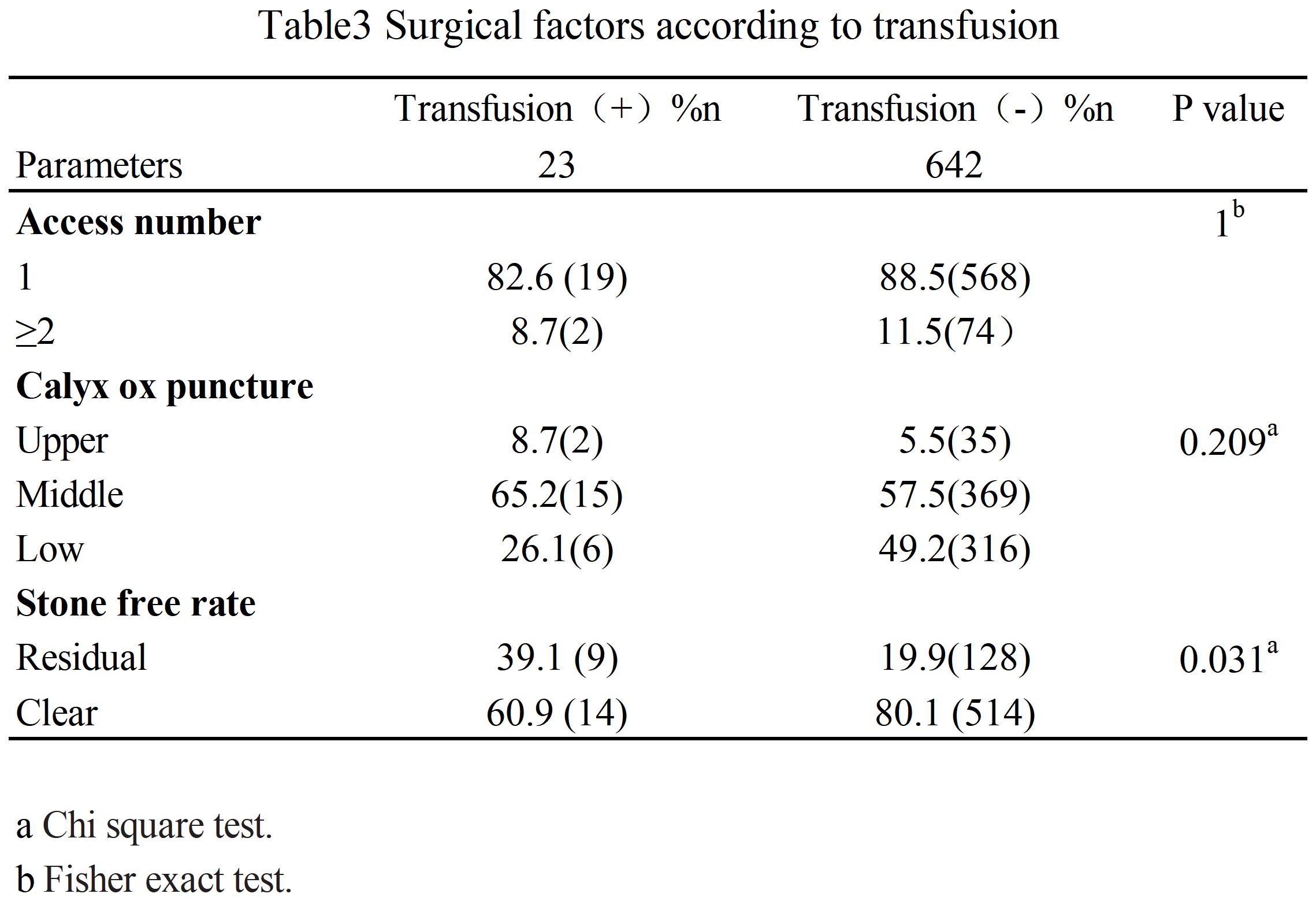
Access number was thought to be associated with bleeding during PCNL. Nevertheless, different study had different results. It may be related to the proportions of multiple tracts of stone removal operations. Arkman and his colleagues [7] found that multiple access surgery increases the risk of bleeding by 2.7 times following PCNL (P < 0.001). In that study, the percent of multiple tract accesses was 22.7%. In another study, Soucy and his colleagues [8] found that there was no statistically significant difference in transfusion rates (0.7–1.2% P = 0.24) in patients who were treated with a single tract or among those needing multiple tracts. In their study, the percent of multiple tract accesses was 16%. In our study, the percent of multiple accesses was 11.5%. There are relatively few patients with multi-channel puncture in our group. Only 74 patients received 2 channels and 2 patients had 3 channels, which would cause data bias. This is one of the limitations of our research.
Renal pelvic perforation is associated with bleeding in our study. The history of open surgery will increase the risk of severe bleeding by 3 times. Patients with a open surgery history may have a different kidney anatomy, and this may increase the risk of bleeding at the puncture site. This result is consistent with Christian’s [6] work. In these six studies, only Arkman[7] demonstrated that bleeding had no relation with previous surgery history following PCNL.
Our study found that preoperative hemoglobin levels were associated with transfusion, consistent with the study reported by Akman’s [7]. Among our bleeding patients, there were 13 patients having preoperative anemia ( average Hb was114.6 g/l), accounting for 56.5% with hemoglobin ranges from 63 g/l to 127g/l. In the non-transfusion group, the preoperatively anaemic rate was 10%. The average Hb loss was 52.9g/l in the transfusion group. Among them, six patients had received a two-stage operation during one hospital stay. For them, hemoglobin before the second operation was 94g/L. Average blood loss was 28.2g/l. For a second-stage PCNL operation patient, if there is anemia before the operation, he will have a higher transfusion rate during PCNL.
Yamaguchi [5], Akman [7], and Srivastava[9] found that the stone load (size) was associated with bleeding during PCNL. Operation time was also associated with bleeding in Yamaguchi [5] and AkmanL’s [7] study. Large stones often mean more puncture tracts and longer operation time. In our study, for staghorn calculi, transfusion was 0.066 compared to non-staghorn ones. Tract establishments were all performed by Dr. G.J.M in this study. He used an 18-gauge needle to access to the selected calyx with the aid of ultrasound guidance. The tract was dilatated with serial dilators from 8F to 20F sheath. The overall process was completed within 5 minutes. With the update of laser technology and stronger lithotripsy efficiency, the operation time can be greatly shortened than before. The operation time is not included in our study, which is a limitation of this study.
The caseload is also associated with bleeding during PCNL. In the CROES study, Opondo [12] and his colleagues found that a high volume center (> 120 cases per year) usually has higher stone-free rates and lower complication rates. In studies reported previously, the transfusion rate was 5.24% vs 3.4 % (P < 0.001) according to low volume center and high volume center.
A positive preoperative urine culture will increase bleeding complications following PCNL in both intraoperative and postoperative hematuria [13]. Despite antibiotic treatment before surgery, urine infection will increase the risk of severe bleeding in PCNL by 16 times. We had found that when infectious stones were seen when access was made into the kidney, indwelling nephrostomy immediately for drainage and stop the surgery is the best measure. Slightly increased operation time and water pressure will increase the risk of bleeding in PCNL.
We used plain abdominal radiography of the kidneys, ureters, and bladder (KUB) or ultrasound for a postoperative image. This test may result in false negative results for stones. But we use postoperative ultrasound or CT to correct this bias. All patients have received a follow-up for at least one year. The total stone-free rate was 79.4% (528/665). For the transfusion group, the SFR was 60.9% (14/23),and in the non-transfusion group༌the SFR was 80.1%(514/642) (P = 0.031). The group of no transfusion was 2.5 times more likely to get rid of the stones than those who suffered serious bleeding in PCNL.
In our study, the blood transfusion rate found was 3.5%. In previously reported literature of more than 500 cases, the blood transfusion rate ranges from 0.8–12.3% [5, 7, 8, 9, 10, 11], So our results were correlated with previous reports. Our center had a low transfusion rate as compared to the reported cases by others. The reason may be attributed to the use of medium tract passage, ultrasound-guided puncture to save time, relatively few puncture tracts and application of high-power laser to fragment stones. In a retrospective study, 305 patients who underwent percutaneous nephrolithotomy, reported a blood transfusion rate of 0%. Their experience is worth learning: Careful patient selection, accurate positioning, and use of the best available instruments with well-trained urologists are necessary to avoid the complications associated with PCNL [14].
In our study we have attempted to analyze PCNL surgery in high-volume center and previous case studies. Although it is a retrospective study, the obtained results demonstrated that PCNL is a safer surgery for an experienced surgeon. For a high-volume urolithiasis center, anemic conditions, infection before the surgery, and the history of open kidney surgery will significantly increase the risk of hemorrhagic complications following PCNL. The operation time was not included in our study as well as the time taken to achieve access into the desired calyx. This is a limitation of the study. In addition, for the follow-up of stones, we use KUB instead of CT. This may bring about a bias of high postoperative success rate. Although we use one year for follow-up after surgery, there will definitely be data bias, but overall, our study might have a ground-breaking interest for the readers about PCNL surgery significance factors affecting bleeding during PCNL.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}