From January 1, 2020 to January 31, 2021, a total of twenty-six implanted Impella 5.5® minimally invasive axial LVADs were identified in 24 hospitalized patients at our institution. Patients’ ages at implant ranged from 20 to 81 years old (Mean of 51 ± 31 years) with 92% identified as male. Average length of Impella 5.5® use was 15 days (± 15) with the longest duration of implantation being 80 days.
The predominant indication for Impella 5.5® support was cardiogenic shock secondary to acute myocardial infarction with 11 instances (46% total). Of those, 10 cases were with ST segment elevation myocardial infarction and 1 case with non-ST segment elevation myocardial infarction in which use was for high-risk percutaneous coronary intervention support. The second most predominant indication was for low output congestive systolic heart failure (33%), followed by cardiotomy (21%). The majority of implants were via right axillary artery regardless of indication (77%). Those implants that were via left axillary artery (7%) were for Impella 5.5® exchange after device malfunction and those that were via direct aortic access (15%) were during cardiotomy.
The overall mortality during index hospitalization was 25%. All deaths were in the setting of acute myocardial infarction or high risk percutaneous coronary intervention. Of the patients in the cohort, 75% survived. Out of those who survived, 83% had recovery of native heart function, 6% underwent cardiac transplantation, and 11% underwent durable LVAD placement (Graph 1).
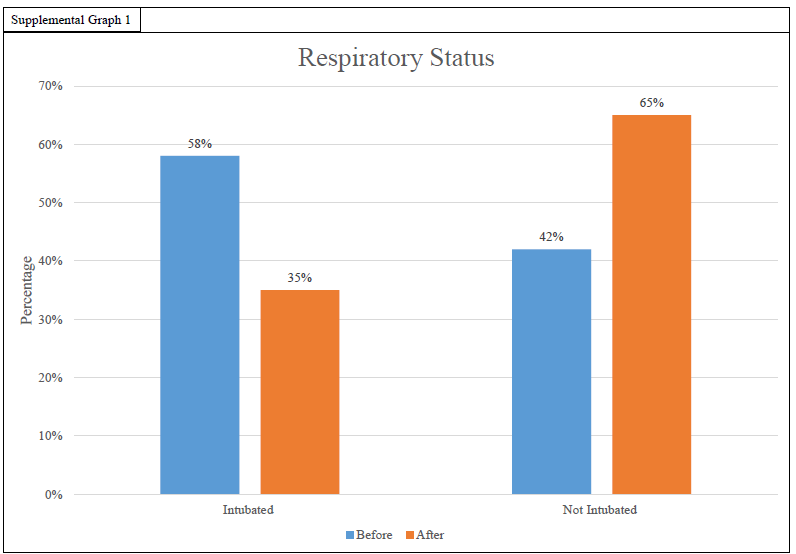
Prior to Impella 5.5® implantation, 58% required mechanical ventilatory support of which 40% were able to be extubated after placement. All patients off mechanical ventilatory support prior to Impella 5.5® placement were able to be extubated post implant. Average time to extubation was 5 (± 5) days post-Impella 5.5® implantation.
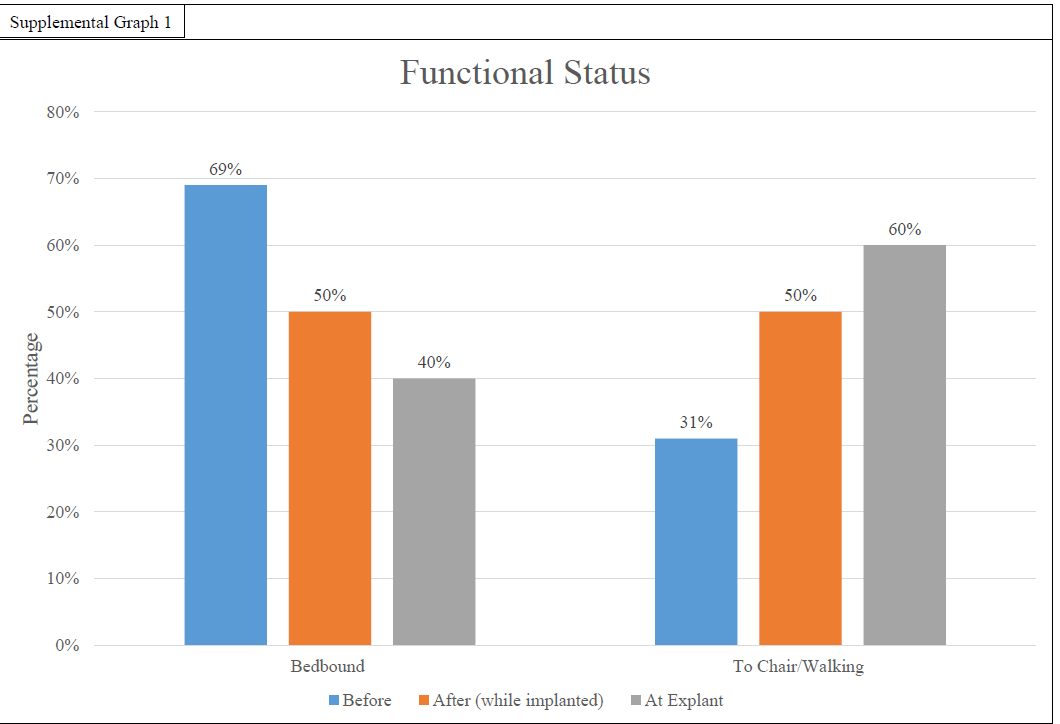
At the time of Impella 5.5® placement, most patients were bed-bound (70%). Of the bed-bound patients after implant, 39% were walking or mobile to bedside chair and post-explant, 50% were walking or mobile to chair.
Invasive hemodynamics were documented on 18 of the patients. Of those patients, CVP improved from an average of 12mmHg (± 6) prior to Impella 5.5® to 8mmHg (± 5) at explant. Mean PA pressure improved from 33mmHg (± 7) to 23mmHg (± 10). Pulmonary artery pulsatility index (PAPi) improved from 2.2 (± 0.7) prior to implant to 5.8 (± 4.9) at explant.
On average, laboratory values showed an improvement in oxygen exchange and end organ function. Of note, mixed venous saturation improved from 54.2% (± 11.8) prior to implantation to 68.8% (± 10.3) at explant. Also, lactate down trended from 4.6 (± 4.0) mmol/L pre-implantation to 1.5 (± 0.6) mmol/L at explant. Using creatinine as a surrogate, kidney function improved after impella 5.5 use. Prior to implantation average creatinine was 1.94 (± 0.79 )mg/dL then after initial increase to 2.0 (± 1.10) mg/dL one day after implantation, creatinine improved to 1.13 (± 0.46) mg/dL at explant. Liver enzymes, aspartate transaminase and alanine transaminase (AST and ALT), saw an initial rise from 442 (± 917) units/L and 503 (± 937) units/L to 354 (± 772) units/L and 548 (± 1362) units/L respectively one day post implant. AST and ALT levels then decreased to 76 (± 86) units/L and 53 (± 55) units/L at time of explant. Hemoglobin overall remained stable with a slight downtrend during implantation from an average of 10.9 (± 2.4) g/dL at implant to 9.6 (± 1.9) g/dL at one day, to ultimately 9.1 (± 1.1) g/dL at explant. Platelets decreased initially with an average of 200,000 (± 127,000) µL at time of implant to 146,000 (± 78,000) µL at day one post implant and 130,000 (± 58,000) µL day five of implant. At the time of explant platelets had improved to 206,000 (± 110,000) µL.
Twenty-three patients received echocardiograms before and after Impella 5.5 implantation during their hospitalization. Improvement in ventricular function was defined as an increase in left ventricular ejection fraction greater than 5% and an improvement in qualitative right ventricular assessment grading of mild, moderate, or severe. Ventricular assessment was taken from the official reports that were finalized during their hospital stay. Ventricular function improved for 39% of patients for the left ventricle and 44% for the right ventricle. Of those with improved left ventricular function, the ejection fraction improved an average of 14% (± 7.7%) (Table 4).
The most common patient complications were gastrointestinal bleeding (15%), axillary hematoma at insertion site (15%), stroke (8%), development of heparin induced thrombocytopenia (8%), and infection at insertion site (4%) (Table 5). All of the axillary hematomas and infections required operative excision, exploration, and washout. One of the gastrointestinal bleedings was severe requiring massive transfusion protocol in which the patient developed acute pulmonary edema, hypoxia, and pulseless electrical activity requiring resuscitation. Ultimately that patient was made comfort measures by the family. There were two instances of device malfunction requiring exchange (8%). One malfunction was a software complication in which the Impella 5.5® device abruptly shut off requiring patient hemodynamic resuscitation and exchange. In that case, the patient survived and was ultimately discharged from the hospital. The other device malfunction was the development of a physical crack in the purge cassette of the Impella 5.5® purge delivery system which had to be temporarily sutured together until a new Impella 5.5® could be exchanged to the left axillary artery. In that case, the patient was successfully hemodynamically stabilized however family ultimately decided to withdraw care instead of having a durable LVAD implanted.
Eleven LVADs in ten patients were identified with an average device implantation for greater than 14 days. Average device implantation for this subgroup was 27 days with a range of 15–80 days. Two of these patients had to undergo an Impella 5.5® re-implantation via the left axillary artery due to device malfunction. Of the subgroup with Impella 5.5® use for greater than 14 days, the median age was 58 with range 20–72 years old. The indication for implantation included cardiogenic shock due to ST-segment elevation myocardial infarction (55%), low output congestive heart failure (36%), and assistance for high-risk percutaneous coronary intervention for non-ST segment elevation myocardial infarction (9%). Complications and rates are listed in Table 5. Survival rate for Impella 5.5® use greater than 14 days was 67%. Of those who survived, 50% had native heart recovery, 17% had durable device implantation, and 33% cardiac transplant. All of the patients who expired were in the setting of cardiogenic shock after acute myocardial infarction. Of the patients who expired, 50% of them were made comfort care after hemodynamic stabilization and goals of care discussions.
Laboratory trends in those patients who had the Impella 5.5® for greater than 14 days were similar to the entire group. Data is listed in the supplemental data section. Overall complications were higher than the comprehensive cohort at 73% over the 46% for the entire cohort.
{kind=link}
{kind=link}